Diploma of Nursing: Case Studies of COPD and Stroke Patients
VerifiedAdded on 2023/06/15
|12
|2548
|299
AI Summary
This article presents two case studies of patients with COPD and stroke, discussing their pathophysiology, symptoms, and treatment. It also highlights the role of allied health professionals in patient care. The article is relevant for students pursuing a Diploma of Nursing.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.

Running head: DIPLOMA OF NURSING
Diploma of nursing
Name of the Student
Name of the University
Author note
Diploma of nursing
Name of the Student
Name of the University
Author note
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
1
DIPLOMA OF NURSING
Part A- Case study of Mr Brown
1.
Mr Brown had past habit of smoking. In lungs oxidative and inflammatory stress
responses occurs with cigarette smoke that in triggers process critical to the development of
COPD. The smoke is viewed as danger by the host and activates the mammalian target of
rapamycin (mTOR). The process of alveolar maintenance is disturbed by oxidative stress,
apoptosis and protease-antiprotease imbalance. A destructive pathway persists even after
smoking cessation and result in structural damage. This initiates emphysema an airflow limited
state (Goldklang & Stockley, 2016).
2.
Low oxygen saturation- is 90 % difficult breathing and due to COPD, restricting
air flow
Blood pressure- resembling hypertension in pulmonary arteries that are
constricted due to hypoxia (Goldklang & Stockley, 2016)
3.
The imbalance between the oxygen demand and supply to heart results in Angina,
characterised by severe chest pain. The increased demand for oxygen is not met due to
obstruction or atherosclerotic plaques and is related with myocardial infarction, and hypertension
in Mr Brown (Ford et al., 2018).
4.
DIPLOMA OF NURSING
Part A- Case study of Mr Brown
1.
Mr Brown had past habit of smoking. In lungs oxidative and inflammatory stress
responses occurs with cigarette smoke that in triggers process critical to the development of
COPD. The smoke is viewed as danger by the host and activates the mammalian target of
rapamycin (mTOR). The process of alveolar maintenance is disturbed by oxidative stress,
apoptosis and protease-antiprotease imbalance. A destructive pathway persists even after
smoking cessation and result in structural damage. This initiates emphysema an airflow limited
state (Goldklang & Stockley, 2016).
2.
Low oxygen saturation- is 90 % difficult breathing and due to COPD, restricting
air flow
Blood pressure- resembling hypertension in pulmonary arteries that are
constricted due to hypoxia (Goldklang & Stockley, 2016)
3.
The imbalance between the oxygen demand and supply to heart results in Angina,
characterised by severe chest pain. The increased demand for oxygen is not met due to
obstruction or atherosclerotic plaques and is related with myocardial infarction, and hypertension
in Mr Brown (Ford et al., 2018).
4.
2
DIPLOMA OF NURSING
Myocardial infarction is caused by the unstable atherosclerotic plaque that disrupts the
vascular endothelium. It is due to formation of intracoronary thrombus which forms the coronary
artery blood flow occlusion. The increase of risk of myocardium necrosis increases with the
coronary occlusion being more proximal. Aldosterone hormone plays a role of damaging the
vascular and myocardial function. As a result it promotes the coronary endothelial dysfunction.
This hormone causes the left ventricular dysfunction and fibrosis followed by progression of
heart failure. Thus, it adversely affects the heart and the blood vessels. It explains the myocardial
infarction and left sided heart failure in Mr Brown. There are five different situations to the
myocardial infarction. In case of Mr. Brown, it is the situation of oxygen supply and demand
imbalance (Kristensen et al., 2015).
5.
One half of the patients with myocardial infarction develop left sided heart failure. Mr
Brown has hypertension. High blood pressure increases the work of left ventricle to pump blood
out of circulatory system. This leads to weakening of heart and heart failure or CCF. With past
myocardial infarction, the process of CCF is enhanced due to coronary artery blood flow
occlusion (Mann & Felker, 2014).
6.
Swollen ankle and legs are related to fluid accumulation in body. It is caused by reduced
blood flow from the heart due to CCF. Since, the fluid does not move back from heart to veins
results in fluid accumulation in lungs, liver, lower limbs and congestion. However, with CCF
the swelling in ankles and legs is obvious (Mann & Felker, 2014).
7.
DIPLOMA OF NURSING
Myocardial infarction is caused by the unstable atherosclerotic plaque that disrupts the
vascular endothelium. It is due to formation of intracoronary thrombus which forms the coronary
artery blood flow occlusion. The increase of risk of myocardium necrosis increases with the
coronary occlusion being more proximal. Aldosterone hormone plays a role of damaging the
vascular and myocardial function. As a result it promotes the coronary endothelial dysfunction.
This hormone causes the left ventricular dysfunction and fibrosis followed by progression of
heart failure. Thus, it adversely affects the heart and the blood vessels. It explains the myocardial
infarction and left sided heart failure in Mr Brown. There are five different situations to the
myocardial infarction. In case of Mr. Brown, it is the situation of oxygen supply and demand
imbalance (Kristensen et al., 2015).
5.
One half of the patients with myocardial infarction develop left sided heart failure. Mr
Brown has hypertension. High blood pressure increases the work of left ventricle to pump blood
out of circulatory system. This leads to weakening of heart and heart failure or CCF. With past
myocardial infarction, the process of CCF is enhanced due to coronary artery blood flow
occlusion (Mann & Felker, 2014).
6.
Swollen ankle and legs are related to fluid accumulation in body. It is caused by reduced
blood flow from the heart due to CCF. Since, the fluid does not move back from heart to veins
results in fluid accumulation in lungs, liver, lower limbs and congestion. However, with CCF
the swelling in ankles and legs is obvious (Mann & Felker, 2014).
7.
3
DIPLOMA OF NURSING
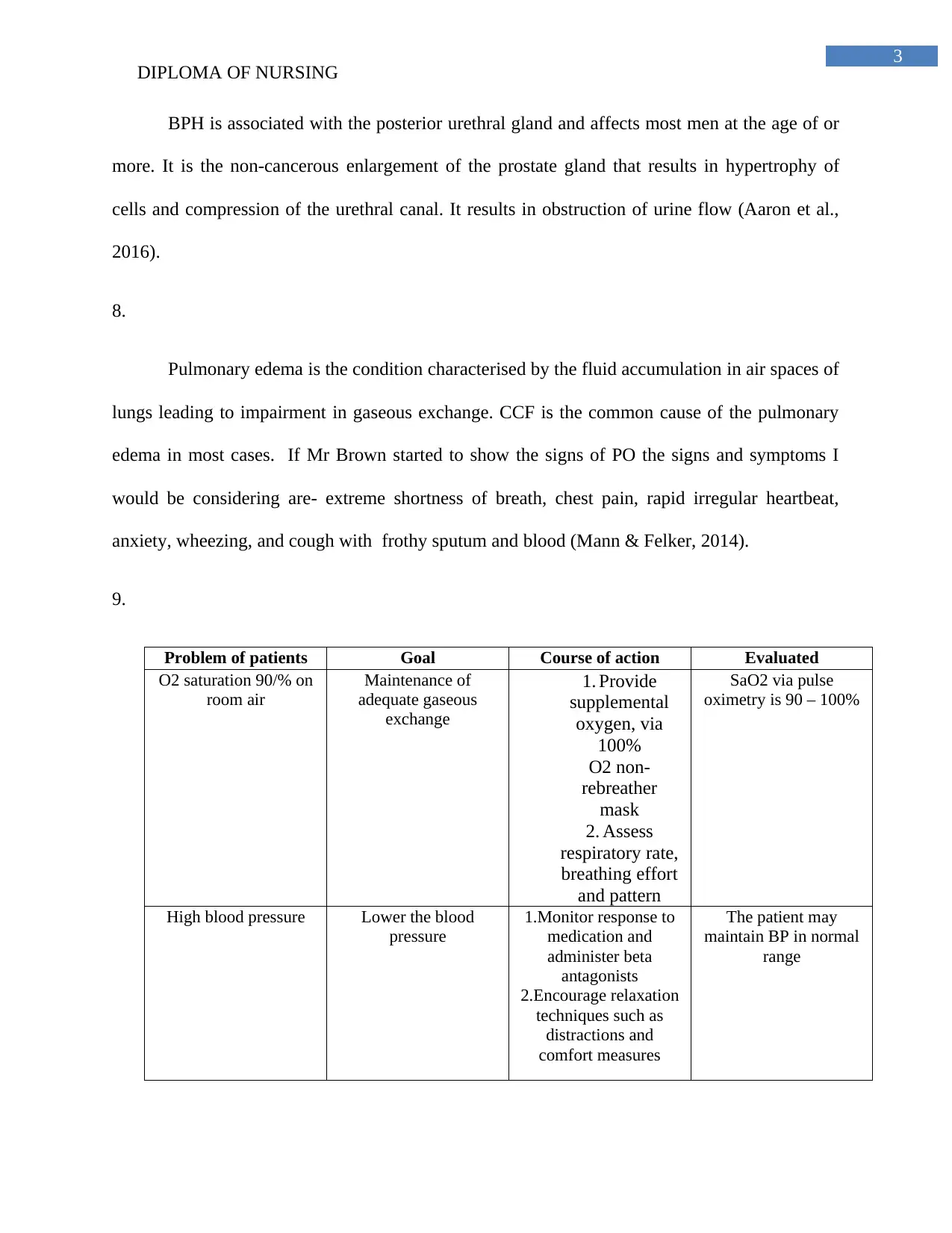
BPH is associated with the posterior urethral gland and affects most men at the age of or
more. It is the non-cancerous enlargement of the prostate gland that results in hypertrophy of
cells and compression of the urethral canal. It results in obstruction of urine flow (Aaron et al.,
2016).
8.
Pulmonary edema is the condition characterised by the fluid accumulation in air spaces of
lungs leading to impairment in gaseous exchange. CCF is the common cause of the pulmonary
edema in most cases. If Mr Brown started to show the signs of PO the signs and symptoms I
would be considering are- extreme shortness of breath, chest pain, rapid irregular heartbeat,
anxiety, wheezing, and cough with frothy sputum and blood (Mann & Felker, 2014).
9.
Problem of patients Goal Course of action Evaluated
O2 saturation 90/% on
room air
Maintenance of
adequate gaseous
exchange
1. Provide
supplemental
oxygen, via
100%
O2 non-
rebreather
mask
2. Assess
respiratory rate,
breathing effort
and pattern
SaO2 via pulse
oximetry is 90 – 100%
High blood pressure Lower the blood
pressure
1.Monitor response to
medication and
administer beta
antagonists
2.Encourage relaxation
techniques such as
distractions and
comfort measures
The patient may
maintain BP in normal
range
DIPLOMA OF NURSING
BPH is associated with the posterior urethral gland and affects most men at the age of or
more. It is the non-cancerous enlargement of the prostate gland that results in hypertrophy of
cells and compression of the urethral canal. It results in obstruction of urine flow (Aaron et al.,
2016).
8.
Pulmonary edema is the condition characterised by the fluid accumulation in air spaces of
lungs leading to impairment in gaseous exchange. CCF is the common cause of the pulmonary
edema in most cases. If Mr Brown started to show the signs of PO the signs and symptoms I
would be considering are- extreme shortness of breath, chest pain, rapid irregular heartbeat,
anxiety, wheezing, and cough with frothy sputum and blood (Mann & Felker, 2014).
9.
Problem of patients Goal Course of action Evaluated
O2 saturation 90/% on
room air
Maintenance of
adequate gaseous
exchange
1. Provide
supplemental
oxygen, via
100%
O2 non-
rebreather
mask
2. Assess
respiratory rate,
breathing effort
and pattern
SaO2 via pulse
oximetry is 90 – 100%
High blood pressure Lower the blood
pressure
1.Monitor response to
medication and
administer beta
antagonists
2.Encourage relaxation
techniques such as
distractions and
comfort measures
The patient may
maintain BP in normal
range
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
4
DIPLOMA OF NURSING
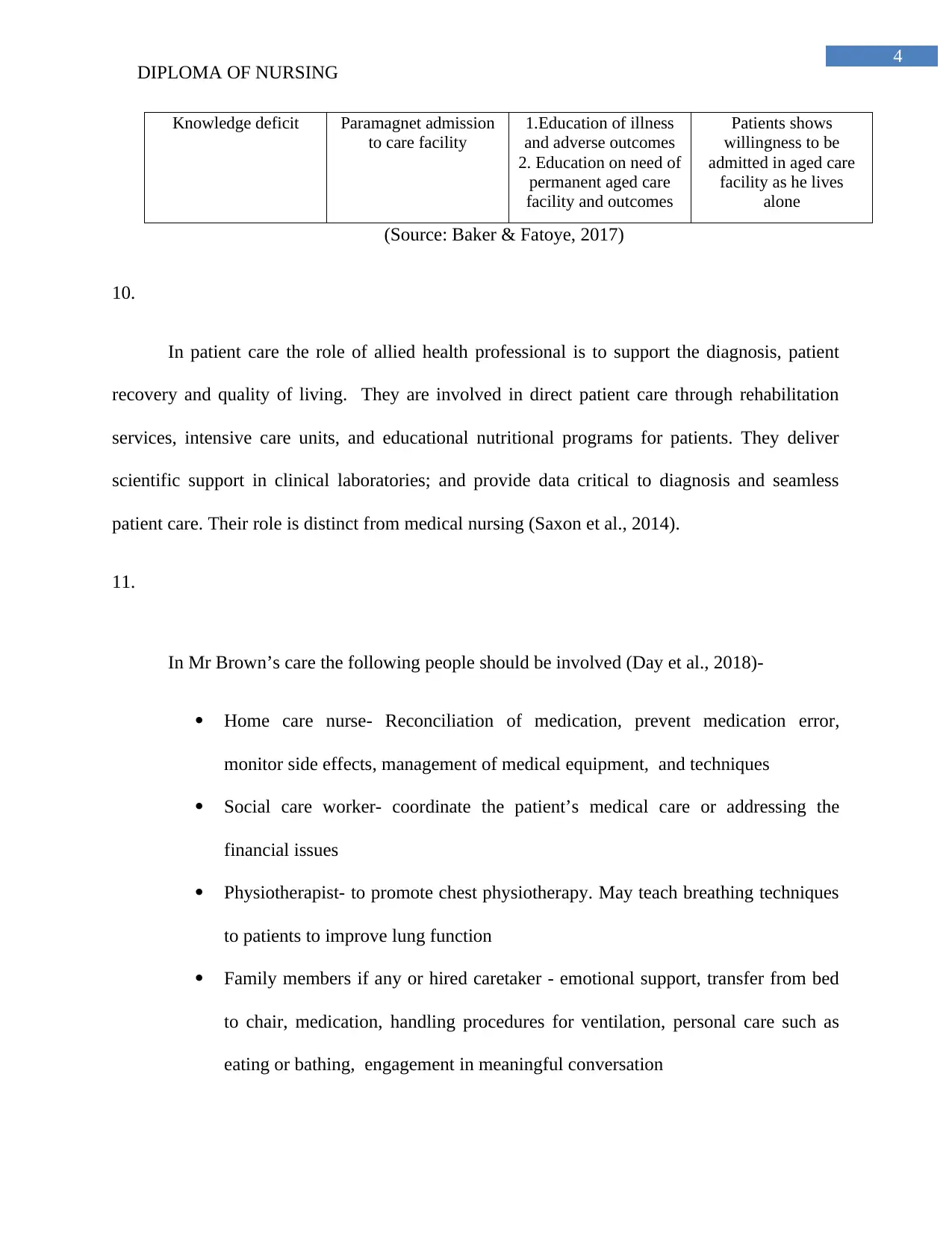
Knowledge deficit Paramagnet admission
to care facility
1.Education of illness
and adverse outcomes
2. Education on need of
permanent aged care
facility and outcomes
Patients shows
willingness to be
admitted in aged care
facility as he lives
alone
(Source: Baker & Fatoye, 2017)
10.
In patient care the role of allied health professional is to support the diagnosis, patient
recovery and quality of living. They are involved in direct patient care through rehabilitation
services, intensive care units, and educational nutritional programs for patients. They deliver
scientific support in clinical laboratories; and provide data critical to diagnosis and seamless
patient care. Their role is distinct from medical nursing (Saxon et al., 2014).
11.
In Mr Brown’s care the following people should be involved (Day et al., 2018)-
Home care nurse- Reconciliation of medication, prevent medication error,
monitor side effects, management of medical equipment, and techniques
Social care worker- coordinate the patient’s medical care or addressing the
financial issues
Physiotherapist- to promote chest physiotherapy. May teach breathing techniques
to patients to improve lung function
Family members if any or hired caretaker - emotional support, transfer from bed
to chair, medication, handling procedures for ventilation, personal care such as
eating or bathing, engagement in meaningful conversation
DIPLOMA OF NURSING
Knowledge deficit Paramagnet admission
to care facility
1.Education of illness
and adverse outcomes
2. Education on need of
permanent aged care
facility and outcomes
Patients shows
willingness to be
admitted in aged care
facility as he lives
alone
(Source: Baker & Fatoye, 2017)
10.
In patient care the role of allied health professional is to support the diagnosis, patient
recovery and quality of living. They are involved in direct patient care through rehabilitation
services, intensive care units, and educational nutritional programs for patients. They deliver
scientific support in clinical laboratories; and provide data critical to diagnosis and seamless
patient care. Their role is distinct from medical nursing (Saxon et al., 2014).
11.
In Mr Brown’s care the following people should be involved (Day et al., 2018)-
Home care nurse- Reconciliation of medication, prevent medication error,
monitor side effects, management of medical equipment, and techniques
Social care worker- coordinate the patient’s medical care or addressing the
financial issues
Physiotherapist- to promote chest physiotherapy. May teach breathing techniques
to patients to improve lung function
Family members if any or hired caretaker - emotional support, transfer from bed
to chair, medication, handling procedures for ventilation, personal care such as
eating or bathing, engagement in meaningful conversation
5
DIPLOMA OF NURSING
Part B- Case study of Jack Jones
1.
In case of TIA the blood flow is blocked to certain part of the brain and the symptoms
may not appear again when flow is restored. In case of stroke the blockage persists and the brain
has permanent damage. The pathophysiology of stroke is the heart disease or underlying damage
of blood vessel. Hyperlipidemia, hypertension, atherosclerosis are the primary pathologies (Amy
& Coutts, 2015).
2.
FAST stands for face, arms, speech, and time and is the immediate action to identify the
stroke patient. Fast means to identify if an individual has face fallen on one side, able to raise
the arms, if the speech is slurred and immediately make a call to emergency care or hospital if
any of these signs are observed (Wolters et al., 2015).
3.
The patient has the high blood pressure of 160/95 and is a matter of concern. Being
hypertension increases the risk of cardiac arrest since the patient already has three TIA’s. With
high blood pressure the patients is at increased risk of morbidity and mortality. It may occur due
to intracranial pressure and variable autonomic stress. An immediate action would be taken to
lower the blood pressure to prevent stroke of TIA (Amy & Coutts, 2015).
4.
The four signs and symptoms Jack may have presented with when diagnosed with
pulmonary embolus or PE are-
DIPLOMA OF NURSING
Part B- Case study of Jack Jones
1.
In case of TIA the blood flow is blocked to certain part of the brain and the symptoms
may not appear again when flow is restored. In case of stroke the blockage persists and the brain
has permanent damage. The pathophysiology of stroke is the heart disease or underlying damage
of blood vessel. Hyperlipidemia, hypertension, atherosclerosis are the primary pathologies (Amy
& Coutts, 2015).
2.
FAST stands for face, arms, speech, and time and is the immediate action to identify the
stroke patient. Fast means to identify if an individual has face fallen on one side, able to raise
the arms, if the speech is slurred and immediately make a call to emergency care or hospital if
any of these signs are observed (Wolters et al., 2015).
3.
The patient has the high blood pressure of 160/95 and is a matter of concern. Being
hypertension increases the risk of cardiac arrest since the patient already has three TIA’s. With
high blood pressure the patients is at increased risk of morbidity and mortality. It may occur due
to intracranial pressure and variable autonomic stress. An immediate action would be taken to
lower the blood pressure to prevent stroke of TIA (Amy & Coutts, 2015).
4.
The four signs and symptoms Jack may have presented with when diagnosed with
pulmonary embolus or PE are-
6
DIPLOMA OF NURSING
1. Tachypnoea, tachycardia-
2. Hypoxia
3. Gallop heart rhythm
4. Elevated jugular venous pressure
Symptoms-
1. Dyspnoea
2. Cough
3. Pleurtic chest pain
4. Dizziness indicating right heat failure (Di Nisio et al., 2016)
5.
Dyspnoea is defined as severe shortness of breath and difficult respiration. Tachycardia is
defined as medical condition where the heart rate is greater than 100 bpm. Haemoptysis is
defined as coughing up of blood from the lungs. Diaphoresis is defined as medical condition of
excess sweating or production of perspiration (Villanueva et al., 2018).
6.
Asthma is characterised by airflow limitations and is caused by various changes such as
bronchoconstriction, airway edema, airway hyperresponsiveness, and airway remodelling. Due
to variety of stimuli such as irritant or allegens, the bronchial smooth muscle contraction occurs,
and limits the air flow. Inflammation becomes more progressive due to edema, and structural
changes such as hypertrophy and hyperplasia. Inflammation, dysfunctional neuroregulation, and
structural changes result in airway hyperresponsiveness. The permanent structural changes in
DIPLOMA OF NURSING
1. Tachypnoea, tachycardia-
2. Hypoxia
3. Gallop heart rhythm
4. Elevated jugular venous pressure
Symptoms-
1. Dyspnoea
2. Cough
3. Pleurtic chest pain
4. Dizziness indicating right heat failure (Di Nisio et al., 2016)
5.
Dyspnoea is defined as severe shortness of breath and difficult respiration. Tachycardia is
defined as medical condition where the heart rate is greater than 100 bpm. Haemoptysis is
defined as coughing up of blood from the lungs. Diaphoresis is defined as medical condition of
excess sweating or production of perspiration (Villanueva et al., 2018).
6.
Asthma is characterised by airflow limitations and is caused by various changes such as
bronchoconstriction, airway edema, airway hyperresponsiveness, and airway remodelling. Due
to variety of stimuli such as irritant or allegens, the bronchial smooth muscle contraction occurs,
and limits the air flow. Inflammation becomes more progressive due to edema, and structural
changes such as hypertrophy and hyperplasia. Inflammation, dysfunctional neuroregulation, and
structural changes result in airway hyperresponsiveness. The permanent structural changes in
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7
DIPLOMA OF NURSING
airway (airway smooth muscle hypertrophy, subepithelial fibrosis, sub-basement membrane, and
hyperplasia) occur due to activation of many structural cells (Killeen & Skora, 2013).
7.
I would position Jack in upright sitting position or high Fowler’s to allow unobstructed
breathing and improve his condition (Chan, 2012).
8.
If Jack has asthma attack then there will be marked changes in HR and RR. The heart rate
increases (more than 120 bpm) during the asthma attack as high cardiac output can combat the
low oxygen in the blood stream. The respiratory rate is also increases due to increase in
breathing owing to narrowing of airways and ventilation perfusion imbalance (Papaiwannou et
al., 2014).
9.
Two allied health workers in case of Jack following stroke are-
1. Physiotherapist- physiotherapy constitutes an important part of rehabilitation after
TIA or stroke. Physiotherapy is important for limb strengthening and relearn the
patterns of movements. The role of physiotherapist is to help patient gain physical
potential and recovery despite the disease severity. It is important for Jack as he
has right sided hemiplegia, dysphasia, and dysphagia (Tamburella et al., 2017).
2. Podiatrist- plays an important role in managing the fall risk in stroke patient. They
also play an important role in cellulitis and diabetic limb salvage. Jack had
DIPLOMA OF NURSING
airway (airway smooth muscle hypertrophy, subepithelial fibrosis, sub-basement membrane, and
hyperplasia) occur due to activation of many structural cells (Killeen & Skora, 2013).
7.
I would position Jack in upright sitting position or high Fowler’s to allow unobstructed
breathing and improve his condition (Chan, 2012).
8.
If Jack has asthma attack then there will be marked changes in HR and RR. The heart rate
increases (more than 120 bpm) during the asthma attack as high cardiac output can combat the
low oxygen in the blood stream. The respiratory rate is also increases due to increase in
breathing owing to narrowing of airways and ventilation perfusion imbalance (Papaiwannou et
al., 2014).
9.
Two allied health workers in case of Jack following stroke are-
1. Physiotherapist- physiotherapy constitutes an important part of rehabilitation after
TIA or stroke. Physiotherapy is important for limb strengthening and relearn the
patterns of movements. The role of physiotherapist is to help patient gain physical
potential and recovery despite the disease severity. It is important for Jack as he
has right sided hemiplegia, dysphasia, and dysphagia (Tamburella et al., 2017).
2. Podiatrist- plays an important role in managing the fall risk in stroke patient. They
also play an important role in cellulitis and diabetic limb salvage. Jack had
8
DIPLOMA OF NURSING
cellulitis two months ago recurrence is expected, therefore, podiatrist is needed to
prevent adverse conditions in future (Torpy & Livingston, 2012).
10.
1. Pleurisy- C
2. Pneumonia- D
3. Artheroscleerosis- E
4. Pneumothorax-A
5. Symptoms of Atrial Fibrillation include- B
DIPLOMA OF NURSING
cellulitis two months ago recurrence is expected, therefore, podiatrist is needed to
prevent adverse conditions in future (Torpy & Livingston, 2012).
10.
1. Pleurisy- C
2. Pneumonia- D
3. Artheroscleerosis- E
4. Pneumothorax-A
5. Symptoms of Atrial Fibrillation include- B
9
DIPLOMA OF NURSING
References
Aaron, L., Franco, O. E., & Hayward, S. W. (2016). Review of prostate anatomy and
embryology and the etiology of benign prostatic hyperplasia. Urologic Clinics, 43(3),
279-288.
Amy, Y. X., & Coutts, S. B. (2015). Stroke: risk assessment to prevent recurrence after mild
stroke or TIA. Nature Reviews Neurology, 11(3), 131.
Baker, E., & Fatoye, F. (2017). Clinical and cost effectiveness of nurse-led self-management
interventions for patients with copd in primary care: A systematic review. International
journal of nursing studies, 71, 125-138.
Chan, Z. C. (2012). Role-playing in the problem-based learning class. Nurse Education in
Practice, 12(1), 21-27.
Day, C. B., Bierhals, C. C. B. K., dos Santos, N. O., Mocellin, D., Predebon, M. L., Dal Pizzol,
F. L. F., & Paskulin, L. M. G. (2018). Nursing home care educational intervention for
family caregivers of older adults post stroke (SHARE): study protocol for a randomised
trial. Trials, 19(1), 96.
Di Nisio, M., van Es, N., & Büller, H. R. (2016). Deep vein thrombosis and pulmonary
embolism. The Lancet, 388(10063), 3060-3073.
Ford, T. J., Corcoran, D., & Berry, C. (2018). Stable coronary syndromes: pathophysiology,
diagnostic advances and therapeutic need. Heart, 104(4), 284-292.
DIPLOMA OF NURSING
References
Aaron, L., Franco, O. E., & Hayward, S. W. (2016). Review of prostate anatomy and
embryology and the etiology of benign prostatic hyperplasia. Urologic Clinics, 43(3),
279-288.
Amy, Y. X., & Coutts, S. B. (2015). Stroke: risk assessment to prevent recurrence after mild
stroke or TIA. Nature Reviews Neurology, 11(3), 131.
Baker, E., & Fatoye, F. (2017). Clinical and cost effectiveness of nurse-led self-management
interventions for patients with copd in primary care: A systematic review. International
journal of nursing studies, 71, 125-138.
Chan, Z. C. (2012). Role-playing in the problem-based learning class. Nurse Education in
Practice, 12(1), 21-27.
Day, C. B., Bierhals, C. C. B. K., dos Santos, N. O., Mocellin, D., Predebon, M. L., Dal Pizzol,
F. L. F., & Paskulin, L. M. G. (2018). Nursing home care educational intervention for
family caregivers of older adults post stroke (SHARE): study protocol for a randomised
trial. Trials, 19(1), 96.
Di Nisio, M., van Es, N., & Büller, H. R. (2016). Deep vein thrombosis and pulmonary
embolism. The Lancet, 388(10063), 3060-3073.
Ford, T. J., Corcoran, D., & Berry, C. (2018). Stable coronary syndromes: pathophysiology,
diagnostic advances and therapeutic need. Heart, 104(4), 284-292.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
10
DIPLOMA OF NURSING
Goldklang, M., & Stockley, R. (2016). Pathophysiology of Emphysema and
Implications. Chronic Obstructive Pulmonary Diseases, 3(1), 454.
Killeen, K., & Skora, E. (2013). Pathophysiology, diagnosis, and clinical assessment of asthma
in the adult. Nursing Clinics, 48(1), 11-23.
Kristensen, S. L., Jhund, P. S., Køber, L., Preiss, D., Kjekshus, J., McKelvie, R. S., ... &
Komajda, M. (2015). Comparison of outcomes after hospitalization for worsening heart
failure, myocardial infarction, and stroke in patients with heart failure and reduced and
preserved ejection fraction. European journal of heart failure, 17(2), 169-176.
Mann, D. L., & Felker, G. M. (2014). Heart Failure E-Book: A Companion to Braunwald's
Heart Disease. Elsevier Health Sciences.
Papaiwannou, A., Zarogoulidis, P., Porpodis, K., Spyratos, D., Kioumis, I., Pitsiou, G., ... &
Tsiouda, T. (2014). Asthma-chronic obstructive pulmonary disease overlap syndrome
(ACOS): current literature review. Journal of thoracic disease, 6(Suppl 1), S146.
Saxon, R. L., Gray, M. A., & Oprescu, F. I. (2014). Extended roles for allied health
professionals: an updated systematic review of the evidence. Journal of multidisciplinary
healthcare, 7, 479.
Tamburella, F., Moreno, J. C., Iosa, M., Pisotta, I., Cincotti, F., Mattia, D., ... & Molinari, M.
(2017). Boosting the traditional physiotherapist approach for stroke spasticity using a
sensorized ankle foot orthosis: a pilot study. Topics in stroke rehabilitation, 24(6), 447-
456.
DIPLOMA OF NURSING
Goldklang, M., & Stockley, R. (2016). Pathophysiology of Emphysema and
Implications. Chronic Obstructive Pulmonary Diseases, 3(1), 454.
Killeen, K., & Skora, E. (2013). Pathophysiology, diagnosis, and clinical assessment of asthma
in the adult. Nursing Clinics, 48(1), 11-23.
Kristensen, S. L., Jhund, P. S., Køber, L., Preiss, D., Kjekshus, J., McKelvie, R. S., ... &
Komajda, M. (2015). Comparison of outcomes after hospitalization for worsening heart
failure, myocardial infarction, and stroke in patients with heart failure and reduced and
preserved ejection fraction. European journal of heart failure, 17(2), 169-176.
Mann, D. L., & Felker, G. M. (2014). Heart Failure E-Book: A Companion to Braunwald's
Heart Disease. Elsevier Health Sciences.
Papaiwannou, A., Zarogoulidis, P., Porpodis, K., Spyratos, D., Kioumis, I., Pitsiou, G., ... &
Tsiouda, T. (2014). Asthma-chronic obstructive pulmonary disease overlap syndrome
(ACOS): current literature review. Journal of thoracic disease, 6(Suppl 1), S146.
Saxon, R. L., Gray, M. A., & Oprescu, F. I. (2014). Extended roles for allied health
professionals: an updated systematic review of the evidence. Journal of multidisciplinary
healthcare, 7, 479.
Tamburella, F., Moreno, J. C., Iosa, M., Pisotta, I., Cincotti, F., Mattia, D., ... & Molinari, M.
(2017). Boosting the traditional physiotherapist approach for stroke spasticity using a
sensorized ankle foot orthosis: a pilot study. Topics in stroke rehabilitation, 24(6), 447-
456.
11
DIPLOMA OF NURSING
Torpy, J. M., & Livingston, E. H. (2012). Health Care Professionals and
Qualifications. Jama, 308(21), 2296-2296.
Villanueva, A., Shaughnessy, G., & Ung, S. (2018, February). 70-Year-Old Woman With
Sudden Onset of Chest Pain and Diaphoresis. In Mayo Clinic Proceedings. Elsevier.
Wolters, F. J., Paul, N. L., Li, L., & Rothwell, P. M. (2015). Sustained impact of UK FAST‐test
public education on response to stroke: a population‐based time‐series
study. International Journal of Stroke, 10(7), 1108-1114.
DIPLOMA OF NURSING
Torpy, J. M., & Livingston, E. H. (2012). Health Care Professionals and
Qualifications. Jama, 308(21), 2296-2296.
Villanueva, A., Shaughnessy, G., & Ung, S. (2018, February). 70-Year-Old Woman With
Sudden Onset of Chest Pain and Diaphoresis. In Mayo Clinic Proceedings. Elsevier.
Wolters, F. J., Paul, N. L., Li, L., & Rothwell, P. M. (2015). Sustained impact of UK FAST‐test
public education on response to stroke: a population‐based time‐series
study. International Journal of Stroke, 10(7), 1108-1114.
1 out of 12
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.