Heart Disease Management and Treatments
VerifiedAdded on 2020/11/23
|15
|2983
|215
Essay
AI Summary
This assignment delves into the multifaceted realm of heart disease management. It examines key risk factors associated with coronary heart disease in Europe, analyzing trends over time. The focus then shifts to contemporary treatment strategies, highlighting the role of evidence-based medications and implantable devices in managing heart failure and respiratory complications. The importance of guideline-directed therapies for heart failure patients before cardioverter-defibrillator implantation is also emphasized. Additionally, the assignment touches upon the psychological impact of heart disease, exploring the connection between post-traumatic stress disorder and incident heart failure, as well as the influence of personality traits on medication adherence.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.
Nursing, Clinical Scenario
Assignment
Assignment
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
TABLE OF CONTENTS
INTRODUCTION...........................................................................................................................1
QUESTION 1...................................................................................................................................1
Rationale for ECG request ..........................................................................................................1
QUESTION 2...................................................................................................................................1
2a. Pathophysiology of angina ....................................................................................................1
2b. Specific risk factors ...............................................................................................................2
QUESTION 3...................................................................................................................................2
ECG interpretation ......................................................................................................................2
QUESTION 4...................................................................................................................................3
Diagnosing Acute coronary syndrome (ACS) ............................................................................3
QUESTION 5...................................................................................................................................4
Drug discussion ...........................................................................................................................4
QUESTION 6...................................................................................................................................6
Action mechanism of ticagrelor and aspirin ...............................................................................6
QUESTION 7...................................................................................................................................6
Benefits and controversies related to Morphine .........................................................................6
QUESTION 8...................................................................................................................................6
Increased depression risk with chronic illness ............................................................................6
CONCLUSION ...............................................................................................................................7
REFERENCES ...............................................................................................................................8
INTRODUCTION...........................................................................................................................1
QUESTION 1...................................................................................................................................1
Rationale for ECG request ..........................................................................................................1
QUESTION 2...................................................................................................................................1
2a. Pathophysiology of angina ....................................................................................................1
2b. Specific risk factors ...............................................................................................................2
QUESTION 3...................................................................................................................................2
ECG interpretation ......................................................................................................................2
QUESTION 4...................................................................................................................................3
Diagnosing Acute coronary syndrome (ACS) ............................................................................3
QUESTION 5...................................................................................................................................4
Drug discussion ...........................................................................................................................4
QUESTION 6...................................................................................................................................6
Action mechanism of ticagrelor and aspirin ...............................................................................6
QUESTION 7...................................................................................................................................6
Benefits and controversies related to Morphine .........................................................................6
QUESTION 8...................................................................................................................................6
Increased depression risk with chronic illness ............................................................................6
CONCLUSION ...............................................................................................................................7
REFERENCES ...............................................................................................................................8
INTRODUCTION
The pathophysiology and pharmacology are closely related to each other and plays
significant role in clinical outcomes. For providing safe and accurate clinical services to patients,
health care service providers monitors the various biological parameters as well as psychosocial
attributes associated with the individua (Roth & et.al., 2016). The study will provide the analysis
and evaluation of clinical scenario of Betsy Blogger. The report will also discuss the angina
pathophysiology and the action, benefits and controversies related to the specific drugs given to
the cardiac patients in reference to the case scenario. Further it will be also analysed in the study
that how chronic illness, medications and treatment procedures leads to depressions and other
psychosocial impacts.
QUESTION 1
Rationale for ECG request
Electrocardiogram, commonly abbreviated as ECG is a clinical diagnosis method which
detects the irregularities in the electrical activities of the heart. Though Betsy did not inform
about any kind of chest pain or discomfort but then also buddy nurse suggested ECG. The key
reason for this suggestion was that many people who have medical history of cardiac diseases are
more vulnerable to heart attack or stroke. The symptoms such as breathing shortness and nausea
are indicators of irregular heart activities which can lead to cardiac arrest in near future. Thus, to
detect any such possibilities or damage to heart muscles ECG test was recommended (Finkel &
et.al., 2018). The ECG result gives information related to heart rhythm, rate and electrical
activities of heart muscles. This data can help to control or eliminate the risk of heart attack.
QUESTION 2
2a. Pathophysiology of angina
The lack of sufficient blood supply to heart muscles causes chest discomfort and the
condition is known as the angina. The difference between myocardial blood supply and demand
of oxygen causes myocardial ischaemia. Thus, epicardial artery is narrowed and impaired
vasodilation and vasoconstriction is caused. The impaired functions of endothelial results in
angina.
There are various types of angina. For instance stable angina or angina pectoris occurs
when heart arteries are blocked or narrowed which is known as the ischemia. On the other hand
unstable angina which is also called ACS can also occur in resting state (Kotseva & et.al., 2017).
1
The pathophysiology and pharmacology are closely related to each other and plays
significant role in clinical outcomes. For providing safe and accurate clinical services to patients,
health care service providers monitors the various biological parameters as well as psychosocial
attributes associated with the individua (Roth & et.al., 2016). The study will provide the analysis
and evaluation of clinical scenario of Betsy Blogger. The report will also discuss the angina
pathophysiology and the action, benefits and controversies related to the specific drugs given to
the cardiac patients in reference to the case scenario. Further it will be also analysed in the study
that how chronic illness, medications and treatment procedures leads to depressions and other
psychosocial impacts.
QUESTION 1
Rationale for ECG request
Electrocardiogram, commonly abbreviated as ECG is a clinical diagnosis method which
detects the irregularities in the electrical activities of the heart. Though Betsy did not inform
about any kind of chest pain or discomfort but then also buddy nurse suggested ECG. The key
reason for this suggestion was that many people who have medical history of cardiac diseases are
more vulnerable to heart attack or stroke. The symptoms such as breathing shortness and nausea
are indicators of irregular heart activities which can lead to cardiac arrest in near future. Thus, to
detect any such possibilities or damage to heart muscles ECG test was recommended (Finkel &
et.al., 2018). The ECG result gives information related to heart rhythm, rate and electrical
activities of heart muscles. This data can help to control or eliminate the risk of heart attack.
QUESTION 2
2a. Pathophysiology of angina
The lack of sufficient blood supply to heart muscles causes chest discomfort and the
condition is known as the angina. The difference between myocardial blood supply and demand
of oxygen causes myocardial ischaemia. Thus, epicardial artery is narrowed and impaired
vasodilation and vasoconstriction is caused. The impaired functions of endothelial results in
angina.
There are various types of angina. For instance stable angina or angina pectoris occurs
when heart arteries are blocked or narrowed which is known as the ischemia. On the other hand
unstable angina which is also called ACS can also occur in resting state (Kotseva & et.al., 2017).
1
It is caused when fatty build up rupture the blood vessels and blood flow is blocked. Another
popular types of ACS are STEMI and non-STEMI. The STEMI heart attack is caused by a
sudden and complete blockage of coronary artery while non-SEEMI is known as process in
which artery is narrowed. STEMI damages are more severe as compare to non-STEMI and needs
quick treatment approaches such as opening of complete artery so that remaining heart can be
prevented from the damage.
2b. Specific risk factors
As per the medical history and current clinical analysis there are certain risk factors
which enhances the possibilities of ACS. The first and prior risk factor is type 2 diabetes
mellitus. Along with the diabetes Betsy also has history of hypertension which elevates the blood
pressure (Krahnke & et.al., 2015). The stress, use of specific medications and other clinical or
biological events can enhance the blood pressure. There has been non linear relation between the
abnormal range of blood glucose levels and ACS. The increased sugar level in the body
increases the microvascular dysfunction and thus myocardial perfusion defect is observed. Betsy
has both the risks and thus her risks of getting affected by acute coronary syndrome. The
individuals suffering from the high blood pressure often face many heart diseases.
QUESTION 3
ECG interpretation
The interpretation of ECG gives the details of parameters related to the electrical activity
of heart. The analysis of these attributes helps health professionals to diagnose the abnormalities
in the functioning of heart.
Rhythm:
The sinus rhythm is the original activities originating from sinus node and is indicated by
upright P wave in second lead on ECG (Rosenbaum, 2015). The analysis of rhythms help to
detect the irregular heart beat sequence so that too fast or too slow heart betas can be determined.
Heart rate
ECG can help to determine atrial and ventricular rates. The frequency of QRS complex
gives the ventricular rate while the atrial rate is obtained by p wave frequency. Betsy has
coronary heart disease both of these heart rates are not identical.
P wave regularity and ST segment
2
popular types of ACS are STEMI and non-STEMI. The STEMI heart attack is caused by a
sudden and complete blockage of coronary artery while non-SEEMI is known as process in
which artery is narrowed. STEMI damages are more severe as compare to non-STEMI and needs
quick treatment approaches such as opening of complete artery so that remaining heart can be
prevented from the damage.
2b. Specific risk factors
As per the medical history and current clinical analysis there are certain risk factors
which enhances the possibilities of ACS. The first and prior risk factor is type 2 diabetes
mellitus. Along with the diabetes Betsy also has history of hypertension which elevates the blood
pressure (Krahnke & et.al., 2015). The stress, use of specific medications and other clinical or
biological events can enhance the blood pressure. There has been non linear relation between the
abnormal range of blood glucose levels and ACS. The increased sugar level in the body
increases the microvascular dysfunction and thus myocardial perfusion defect is observed. Betsy
has both the risks and thus her risks of getting affected by acute coronary syndrome. The
individuals suffering from the high blood pressure often face many heart diseases.
QUESTION 3
ECG interpretation
The interpretation of ECG gives the details of parameters related to the electrical activity
of heart. The analysis of these attributes helps health professionals to diagnose the abnormalities
in the functioning of heart.
Rhythm:
The sinus rhythm is the original activities originating from sinus node and is indicated by
upright P wave in second lead on ECG (Rosenbaum, 2015). The analysis of rhythms help to
detect the irregular heart beat sequence so that too fast or too slow heart betas can be determined.
Heart rate
ECG can help to determine atrial and ventricular rates. The frequency of QRS complex
gives the ventricular rate while the atrial rate is obtained by p wave frequency. Betsy has
coronary heart disease both of these heart rates are not identical.
P wave regularity and ST segment
2
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
P wave on ECG is followed by QRS and T wave. The p wave deflection is related to
atrial depolarisation with amplitude of range 0.05-0.25 mV. The clinicians usually prefer V1 lead
to analyse these waves as its provides the constant contour of P wave. The normal p wave is
round and upright. For analysis of ventricular repolarization in the initial phases is represented
by ST segment. The normal ST segment is an isoelectric line whose elevation and depressions
gives critical findings.
ECG interpretation
In the given ECG location of ST elevation can be used to determine the infarct while the
depression can be used to find out the ischemia. For determining the heart rate R-R duration is
divided by 60. The normal sinus rhythem is in the range 60-100 and thus is normal. The p wave
contour has peak voltage and thus it indicates atrial hypertrophy.
QUESTION 4
Diagnosing Acute coronary syndrome (ACS)
ACS is refers to abnormal physiological changes in which the insufficient blood flow in
coronary arteries cause improper functioning of heart muscles. The muscles can even die and is
characterised by symptoms such as sweating, nausea and chest pain. The central findings which
confirms the diagnosis of ACS are as follows:
Electrocardiogram readings
ECG provides the live image of the heart and thus heart activity can be monitored and
ACS can be diagnosed. The ECG observations provides the elevations of ST segment, pulse rate
and heart rhythm (Kim & et.al., 2016). It can also help to distinguish between NSTEMI and
angina and to confirm the immediate needs of angioplasty or other measurements.
Cardiac troponin biomarker
The analysis of desirable values of enzymes such as troponin, CK-MB can provides the
confirmation for the myocardial infarction and thus is widely used as biomarker for the diagnosis
of ACS.
Blood test and imaging
The blood test can give details of cardiac enzymes, C-reactive protein, prothrombin and
homocysteine. It helps professionals to determine the extent of damage caused to heart muscles
as well as to assess the risk of blood clot or coronary disease (Ponikowski & et.al., 2016). Blood
test also reveals if heart muscles are dying so that ACS can be detected. Along with this test
3
atrial depolarisation with amplitude of range 0.05-0.25 mV. The clinicians usually prefer V1 lead
to analyse these waves as its provides the constant contour of P wave. The normal p wave is
round and upright. For analysis of ventricular repolarization in the initial phases is represented
by ST segment. The normal ST segment is an isoelectric line whose elevation and depressions
gives critical findings.
ECG interpretation
In the given ECG location of ST elevation can be used to determine the infarct while the
depression can be used to find out the ischemia. For determining the heart rate R-R duration is
divided by 60. The normal sinus rhythem is in the range 60-100 and thus is normal. The p wave
contour has peak voltage and thus it indicates atrial hypertrophy.
QUESTION 4
Diagnosing Acute coronary syndrome (ACS)
ACS is refers to abnormal physiological changes in which the insufficient blood flow in
coronary arteries cause improper functioning of heart muscles. The muscles can even die and is
characterised by symptoms such as sweating, nausea and chest pain. The central findings which
confirms the diagnosis of ACS are as follows:
Electrocardiogram readings
ECG provides the live image of the heart and thus heart activity can be monitored and
ACS can be diagnosed. The ECG observations provides the elevations of ST segment, pulse rate
and heart rhythm (Kim & et.al., 2016). It can also help to distinguish between NSTEMI and
angina and to confirm the immediate needs of angioplasty or other measurements.
Cardiac troponin biomarker
The analysis of desirable values of enzymes such as troponin, CK-MB can provides the
confirmation for the myocardial infarction and thus is widely used as biomarker for the diagnosis
of ACS.
Blood test and imaging
The blood test can give details of cardiac enzymes, C-reactive protein, prothrombin and
homocysteine. It helps professionals to determine the extent of damage caused to heart muscles
as well as to assess the risk of blood clot or coronary disease (Ponikowski & et.al., 2016). Blood
test also reveals if heart muscles are dying so that ACS can be detected. Along with this test
3
angiogram rays can also be used to view t he blood vessels image and thus cardiac
catheterization is performed.
QUESTION 5
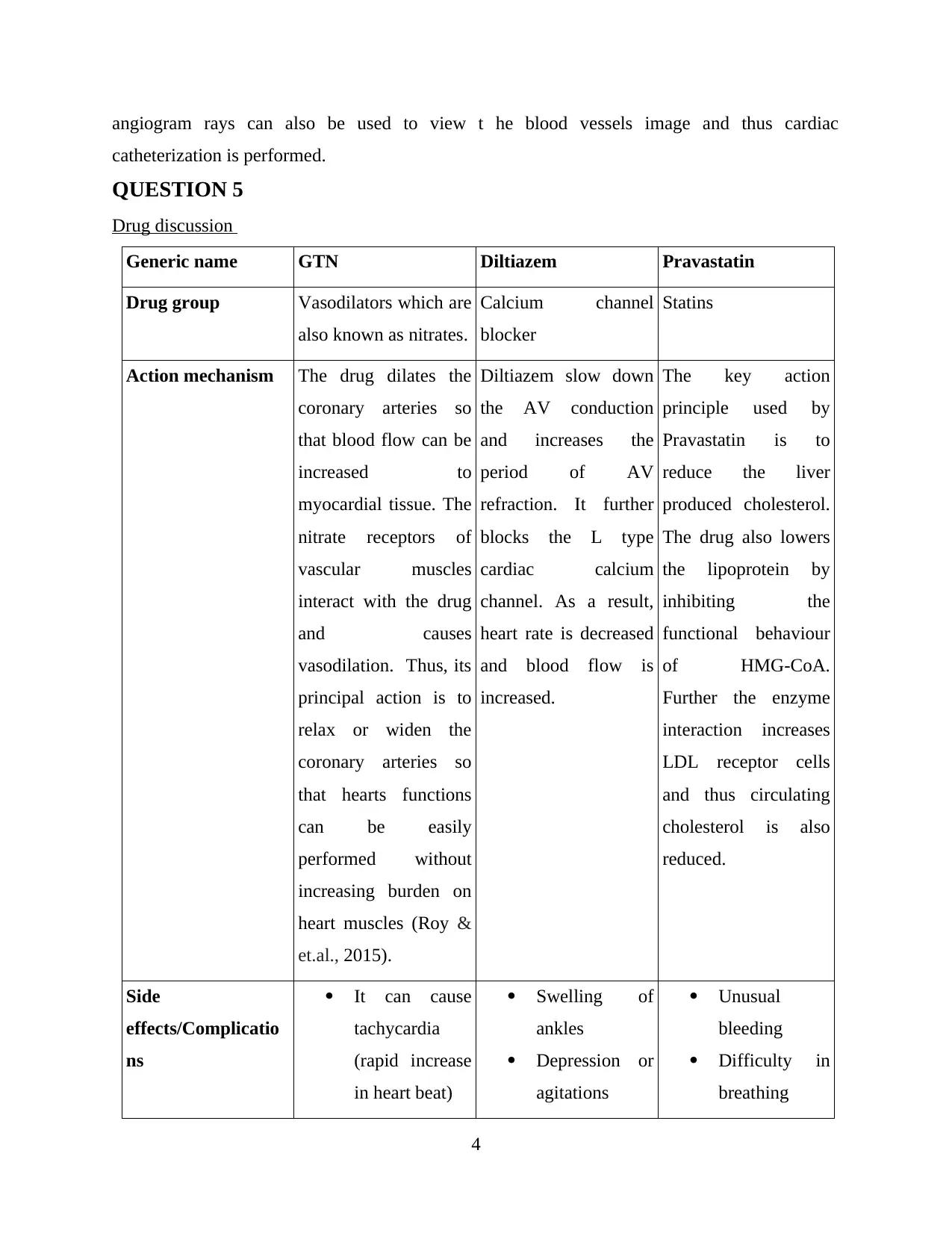
Drug discussion
Generic name GTN Diltiazem Pravastatin
Drug group Vasodilators which are
also known as nitrates.
Calcium channel
blocker
Statins
Action mechanism The drug dilates the
coronary arteries so
that blood flow can be
increased to
myocardial tissue. The
nitrate receptors of
vascular muscles
interact with the drug
and causes
vasodilation. Thus, its
principal action is to
relax or widen the
coronary arteries so
that hearts functions
can be easily
performed without
increasing burden on
heart muscles (Roy &
et.al., 2015).
Diltiazem slow down
the AV conduction
and increases the
period of AV
refraction. It further
blocks the L type
cardiac calcium
channel. As a result,
heart rate is decreased
and blood flow is
increased.
The key action
principle used by
Pravastatin is to
reduce the liver
produced cholesterol.
The drug also lowers
the lipoprotein by
inhibiting the
functional behaviour
of HMG-CoA.
Further the enzyme
interaction increases
LDL receptor cells
and thus circulating
cholesterol is also
reduced.
Side
effects/Complicatio
ns
It can cause
tachycardia
(rapid increase
in heart beat)
Swelling of
ankles
Depression or
agitations
Unusual
bleeding
Difficulty in
breathing
4
catheterization is performed.
QUESTION 5
Drug discussion
Generic name GTN Diltiazem Pravastatin
Drug group Vasodilators which are
also known as nitrates.
Calcium channel
blocker
Statins
Action mechanism The drug dilates the
coronary arteries so
that blood flow can be
increased to
myocardial tissue. The
nitrate receptors of
vascular muscles
interact with the drug
and causes
vasodilation. Thus, its
principal action is to
relax or widen the
coronary arteries so
that hearts functions
can be easily
performed without
increasing burden on
heart muscles (Roy &
et.al., 2015).
Diltiazem slow down
the AV conduction
and increases the
period of AV
refraction. It further
blocks the L type
cardiac calcium
channel. As a result,
heart rate is decreased
and blood flow is
increased.
The key action
principle used by
Pravastatin is to
reduce the liver
produced cholesterol.
The drug also lowers
the lipoprotein by
inhibiting the
functional behaviour
of HMG-CoA.
Further the enzyme
interaction increases
LDL receptor cells
and thus circulating
cholesterol is also
reduced.
Side
effects/Complicatio
ns
It can cause
tachycardia
(rapid increase
in heart beat)
Swelling of
ankles
Depression or
agitations
Unusual
bleeding
Difficulty in
breathing
4
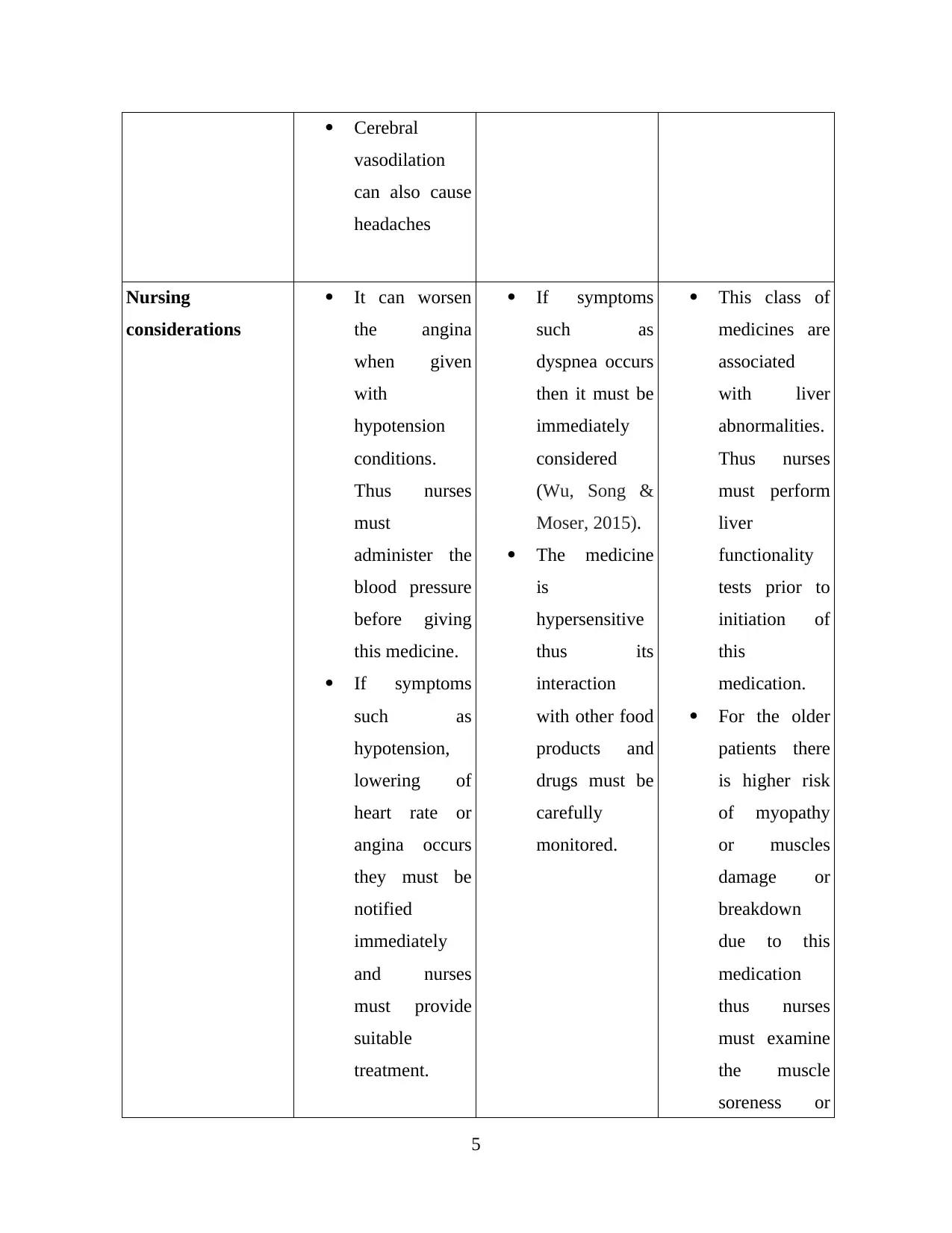
Cerebral
vasodilation
can also cause
headaches
Nursing
considerations
It can worsen
the angina
when given
with
hypotension
conditions.
Thus nurses
must
administer the
blood pressure
before giving
this medicine.
If symptoms
such as
hypotension,
lowering of
heart rate or
angina occurs
they must be
notified
immediately
and nurses
must provide
suitable
treatment.
If symptoms
such as
dyspnea occurs
then it must be
immediately
considered
(Wu, Song &
Moser, 2015).
The medicine
is
hypersensitive
thus its
interaction
with other food
products and
drugs must be
carefully
monitored.
This class of
medicines are
associated
with liver
abnormalities.
Thus nurses
must perform
liver
functionality
tests prior to
initiation of
this
medication.
For the older
patients there
is higher risk
of myopathy
or muscles
damage or
breakdown
due to this
medication
thus nurses
must examine
the muscle
soreness or
5
vasodilation
can also cause
headaches
Nursing
considerations
It can worsen
the angina
when given
with
hypotension
conditions.
Thus nurses
must
administer the
blood pressure
before giving
this medicine.
If symptoms
such as
hypotension,
lowering of
heart rate or
angina occurs
they must be
notified
immediately
and nurses
must provide
suitable
treatment.
If symptoms
such as
dyspnea occurs
then it must be
immediately
considered
(Wu, Song &
Moser, 2015).
The medicine
is
hypersensitive
thus its
interaction
with other food
products and
drugs must be
carefully
monitored.
This class of
medicines are
associated
with liver
abnormalities.
Thus nurses
must perform
liver
functionality
tests prior to
initiation of
this
medication.
For the older
patients there
is higher risk
of myopathy
or muscles
damage or
breakdown
due to this
medication
thus nurses
must examine
the muscle
soreness or
5
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
weakness
experienced
by patient.
QUESTION 6
Action mechanism of ticagrelor and aspirin
The action mechanism of ticagrelor is serving as an allosteric antagonist which blocks the
ADP receptors. The blocking action of the drug is reversible and does not require hepatic
activation. Along with this aspirin is also used for the cardiovascular diseases. Aspirin works on
the principle of platelet aggregation and activation (Dai & Ge., 2011). Another action
mechanism used by aspirin is that it decreases inflammatory response in COPD patients by
improving vasodilation.
Clinicians prefers combining aspiring with ticagrelor as it significantly lowers the risk of
further heart attack or stroke. The solely use of aspirin or ticagrelor have higher risk of blood clot
or internal bleeding. Their combination controls the higher dosage of medication and thus other
complications like blood clot or stroke are prevented.
QUESTION 7
Benefits and controversies related to Morphine
Morphine is used for the treatment of moderate to severe pain. The medication is also
preferred for the treatment of the pain generated due to myocardial infarction and pulmonary
edema. Another benefit of using morphine is that it can increase the mortality in event of Non
STEMI. However, there has been certain controversies are associated with the long term use of
morphine.
The key controversy associated with the long term use of morphine is its ability to
develop physical dependency. Thus, its consumption can make individuals addictive. The drug
abuse and addiction disorders are the most common adverse impact and controversies related to
this drug (Jeannette, 2016). Further the over dose of medicine can also cause respiratory
depression and asphyxia or can even lead to death.
6
experienced
by patient.
QUESTION 6
Action mechanism of ticagrelor and aspirin
The action mechanism of ticagrelor is serving as an allosteric antagonist which blocks the
ADP receptors. The blocking action of the drug is reversible and does not require hepatic
activation. Along with this aspirin is also used for the cardiovascular diseases. Aspirin works on
the principle of platelet aggregation and activation (Dai & Ge., 2011). Another action
mechanism used by aspirin is that it decreases inflammatory response in COPD patients by
improving vasodilation.
Clinicians prefers combining aspiring with ticagrelor as it significantly lowers the risk of
further heart attack or stroke. The solely use of aspirin or ticagrelor have higher risk of blood clot
or internal bleeding. Their combination controls the higher dosage of medication and thus other
complications like blood clot or stroke are prevented.
QUESTION 7
Benefits and controversies related to Morphine
Morphine is used for the treatment of moderate to severe pain. The medication is also
preferred for the treatment of the pain generated due to myocardial infarction and pulmonary
edema. Another benefit of using morphine is that it can increase the mortality in event of Non
STEMI. However, there has been certain controversies are associated with the long term use of
morphine.
The key controversy associated with the long term use of morphine is its ability to
develop physical dependency. Thus, its consumption can make individuals addictive. The drug
abuse and addiction disorders are the most common adverse impact and controversies related to
this drug (Jeannette, 2016). Further the over dose of medicine can also cause respiratory
depression and asphyxia or can even lead to death.
6
QUESTION 8
Increased depression risk with chronic illness
Depression is defined as the psychological disorder which is characterised by mood
swings, anxiety, loss of interests and loneliness. It is one of the most serious and vulnerable
complication of chronic diseases. Betsy has been sufferer of heart disease for more than eight
years and thus her life has been influenced greatly by treatment procedures, medication and
pathological changes. The use of some specific cardiac medications can cause memory loss,
confusion and other mental illness which can make patient worried. The long battle with the
chronic disease which assumes to have long termed impact through the life makes person
emotionally weaker. Thus, there are higher chances despite having great family support Betsy
may experience depression.
The clinical management of the chronic diseases also needs life style changes. For
example Betsy has medical history of diabetes and symptoms of angina. Thus, she has to focus
on weight management and healthy food intake which has low cholesterol or fat. Thus, it can
make her feel sad that she cannot live her life without continuous clinical interruptions. Also, the
painful therapies for the disease management and physical suffering can weaken the mental
strength of the person (Pujades-Rodriguez & et.al., 2016). It is required that health care
professionals must also analyse and focus on mental health care of the patients suffering from
chronic illness.
CONCLUSION
It can be concluded from the report that nurses must apply their knowledge of
pathophysiology into clinical considerations. It will help them to develop more accurate and
effective medication plan and clinical management strategies. It has been also analysed from the
study that medications such as aspirin, ticagrelor and morphine, GTN and diltiazem which are
widely used for the treatment of cardiac diseases may have side effects. Thus, for assuring the
safety of patients these medicines must be administered carefully. From the above discussion it
can also be concluded that management of chronic disease can also have critical impact on
psychological aspects of patient thus nurses must also include this vulnerability in their clinical
management plan.
7
Increased depression risk with chronic illness
Depression is defined as the psychological disorder which is characterised by mood
swings, anxiety, loss of interests and loneliness. It is one of the most serious and vulnerable
complication of chronic diseases. Betsy has been sufferer of heart disease for more than eight
years and thus her life has been influenced greatly by treatment procedures, medication and
pathological changes. The use of some specific cardiac medications can cause memory loss,
confusion and other mental illness which can make patient worried. The long battle with the
chronic disease which assumes to have long termed impact through the life makes person
emotionally weaker. Thus, there are higher chances despite having great family support Betsy
may experience depression.
The clinical management of the chronic diseases also needs life style changes. For
example Betsy has medical history of diabetes and symptoms of angina. Thus, she has to focus
on weight management and healthy food intake which has low cholesterol or fat. Thus, it can
make her feel sad that she cannot live her life without continuous clinical interruptions. Also, the
painful therapies for the disease management and physical suffering can weaken the mental
strength of the person (Pujades-Rodriguez & et.al., 2016). It is required that health care
professionals must also analyse and focus on mental health care of the patients suffering from
chronic illness.
CONCLUSION
It can be concluded from the report that nurses must apply their knowledge of
pathophysiology into clinical considerations. It will help them to develop more accurate and
effective medication plan and clinical management strategies. It has been also analysed from the
study that medications such as aspirin, ticagrelor and morphine, GTN and diltiazem which are
widely used for the treatment of cardiac diseases may have side effects. Thus, for assuring the
safety of patients these medicines must be administered carefully. From the above discussion it
can also be concluded that management of chronic disease can also have critical impact on
psychological aspects of patient thus nurses must also include this vulnerability in their clinical
management plan.
7

8
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
REFERENCES
Books and Journals
Finkel, R. S. & et.al., (2018). Diagnosis and management of spinal muscular atrophy: Part 2:
Pulmonary and acute care; medications, supplements and immunizations; other organ
systems; and ethics. Neuromuscular Disorders. 28(3). 197-207.
Kim, S. & et.al., (2016). Medication adherence and the risk of cardiovascular mortality and
hospitalization among patients with newly prescribed antihypertensive
medications. Hypertension. 67(3). 506-512.
Kotseva, K. & et.al., (2017). Time trends in lifestyle, risk factor control, and use of evidence-
based medications in patients with coronary heart disease in Europe: Results from 3
EUROASPIRE surveys, 1999–2013. Global heart. 12(4). 315-322.
Krahnke, J. S. & et.al., (2015). Heart failure and respiratory hospitalizations are reduced in
patients with heart failure and chronic obstructive pulmonary disease with the use of an
implantable pulmonary artery pressure monitoring device. Journal of cardiac
failure. 21(3). 240-249.
Ponikowski, P. & et.al., (2016). 2016 ESC Guidelines for the diagnosis and treatment of acute
and chronic heart failure: The Task Force for the diagnosis and treatment of acute and
chronic heart failure of the European Society of Cardiology (ESC). Developed with the
special contribution of the Heart Failure Association (HFA) of the ESC. European
journal of heart failure. 18(8). 891-975.
Pujades-Rodriguez, M. & et.al., (2016). Associations between polymyalgia rheumatica and giant
cell arteritis and 12 cardiovascular diseases. Heart. 102(5). 383-389.
Rosenbaum, L. (2015). Beyond belief—how people feel about taking medications for heart
disease.
Roth, G. A. & et.al., (2016). Use of guideline-directed medications for heart failure before
cardioverter-defibrillator implantation. Journal of the American College of
Cardiology. 67(9). 1062-1069.
Roy, S. S. & et.al., (2015). Posttraumatic stress disorder and incident heart failure among a
community-based sample of US veterans. American journal of public health. 105(4).
757-763.
9
Books and Journals
Finkel, R. S. & et.al., (2018). Diagnosis and management of spinal muscular atrophy: Part 2:
Pulmonary and acute care; medications, supplements and immunizations; other organ
systems; and ethics. Neuromuscular Disorders. 28(3). 197-207.
Kim, S. & et.al., (2016). Medication adherence and the risk of cardiovascular mortality and
hospitalization among patients with newly prescribed antihypertensive
medications. Hypertension. 67(3). 506-512.
Kotseva, K. & et.al., (2017). Time trends in lifestyle, risk factor control, and use of evidence-
based medications in patients with coronary heart disease in Europe: Results from 3
EUROASPIRE surveys, 1999–2013. Global heart. 12(4). 315-322.
Krahnke, J. S. & et.al., (2015). Heart failure and respiratory hospitalizations are reduced in
patients with heart failure and chronic obstructive pulmonary disease with the use of an
implantable pulmonary artery pressure monitoring device. Journal of cardiac
failure. 21(3). 240-249.
Ponikowski, P. & et.al., (2016). 2016 ESC Guidelines for the diagnosis and treatment of acute
and chronic heart failure: The Task Force for the diagnosis and treatment of acute and
chronic heart failure of the European Society of Cardiology (ESC). Developed with the
special contribution of the Heart Failure Association (HFA) of the ESC. European
journal of heart failure. 18(8). 891-975.
Pujades-Rodriguez, M. & et.al., (2016). Associations between polymyalgia rheumatica and giant
cell arteritis and 12 cardiovascular diseases. Heart. 102(5). 383-389.
Rosenbaum, L. (2015). Beyond belief—how people feel about taking medications for heart
disease.
Roth, G. A. & et.al., (2016). Use of guideline-directed medications for heart failure before
cardioverter-defibrillator implantation. Journal of the American College of
Cardiology. 67(9). 1062-1069.
Roy, S. S. & et.al., (2015). Posttraumatic stress disorder and incident heart failure among a
community-based sample of US veterans. American journal of public health. 105(4).
757-763.
9
Wu, J. R., Song, E. K. & Moser, D. K. (2015). Type D personality, self-efficacy, and medication
adherence in patients with heart failure—A mediation analysis. Heart & Lung. 44(4).
276-281.
Online
Dai., Y. & Ge., J., (2011). Clinical use of Aspirin in treatment and prevention of Cardiovascular
disease. [Online]. Accessed through
<https://www.hindawi.com/journals/thrombosis/2012/245037/>
Jeannette Y. Wick., (2016). Morphine for myocardial infarction: Pros and cons. [Online].
Accessed through <https://www.pharmacytimes.com/resource-centers/acs/morphine-for-
myocardial-infarction-pros-and-cons>
10
adherence in patients with heart failure—A mediation analysis. Heart & Lung. 44(4).
276-281.
Online
Dai., Y. & Ge., J., (2011). Clinical use of Aspirin in treatment and prevention of Cardiovascular
disease. [Online]. Accessed through
<https://www.hindawi.com/journals/thrombosis/2012/245037/>
Jeannette Y. Wick., (2016). Morphine for myocardial infarction: Pros and cons. [Online].
Accessed through <https://www.pharmacytimes.com/resource-centers/acs/morphine-for-
myocardial-infarction-pros-and-cons>
10

11
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

12

13
1 out of 15
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.