Pathophysiology of Ischemic Stroke: Risk Factors, Diagnosis, and Treatment
VerifiedAdded on 2023/01/16
|4
|1434
|38
Presentation
AI Summary
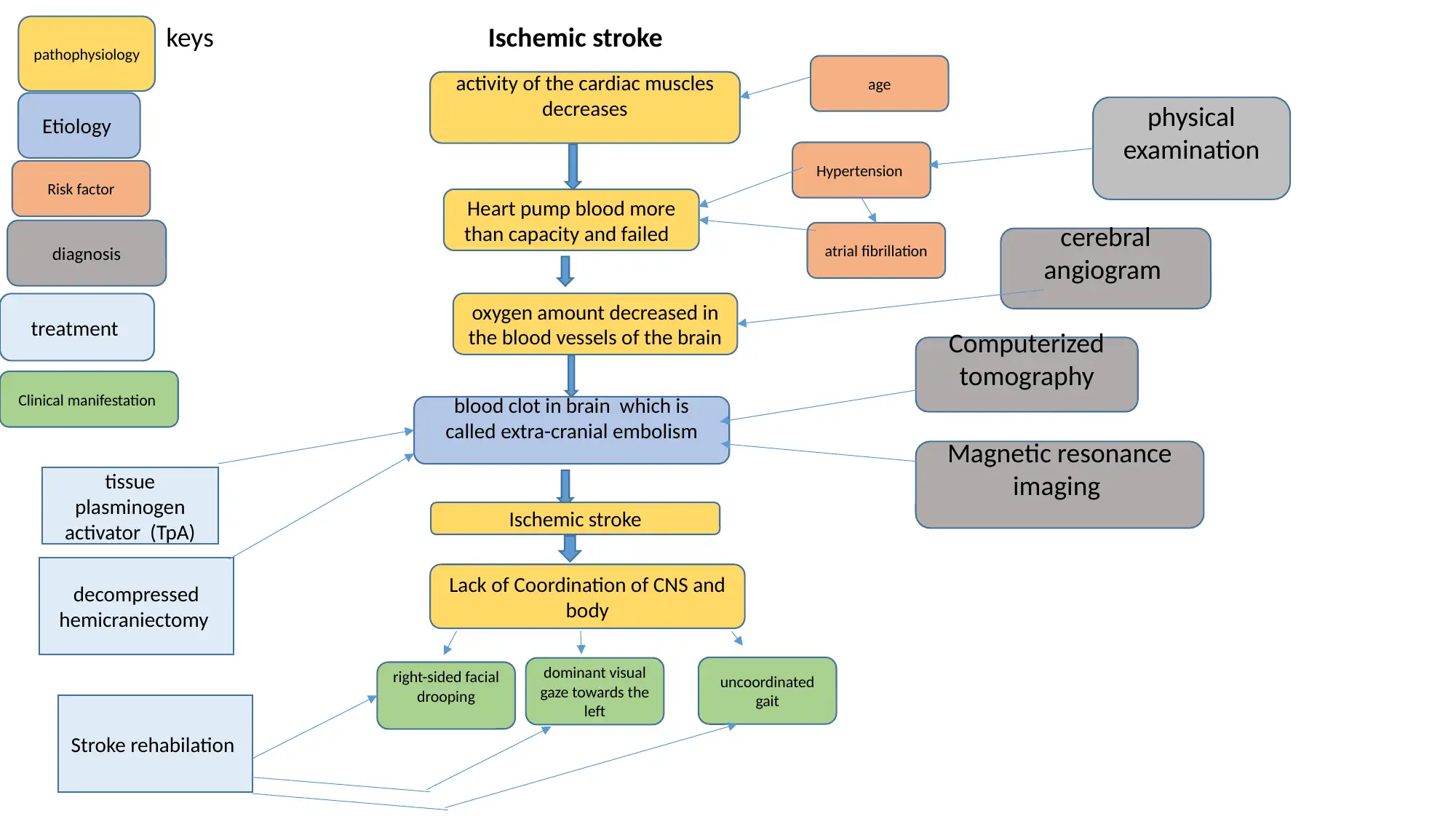
This presentation discusses the pathophysiology of ischemic stroke, including the risk factors, diagnosis, and treatment. It explores the role of hypertension, atrial fibrillation, and age as risk factors for stroke. The diagnostic techniques of CT scan, MRI, and cerebral angiogram are discussed, along with the emergency endovascular procedures and stroke rehabilitation for treatment.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.
1 out of 4
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
© 2024 | Zucol Services PVT LTD | All rights reserved.