Case Study: Plantar Plate Tear in Healthcare - Analysis
VerifiedAdded on 2021/06/17
|15
|2943
|122
Case Study
AI Summary
This case study presents a comprehensive analysis of plantar plate tear, a common forefoot condition. It begins with background information, including the pathophysiology of plantar plate tears, risk factors, and epidemiology. The case study details a patient's subjective and objective history, including physical examination findings, such as the Lachman's test and imaging results. It explores differential diagnoses, assessment methods, and grading systems. The assignment then delves into various management and intervention strategies, including non-operative interventions like footwear modification, anti-inflammatory medicines, stretching, and orthoses, as well as operative management options. The case study also discusses health outcome measures, specifically the Foot and Ankle Ability Measure (FAAM), and concludes with a review of relevant references.

Running Head: CASE STUDY ON PATHOPHYSIOLOGY
0
Case study
Student Name
0
Case study
Student Name
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
CASE STUDY ON PATHOPHYSIOLOGY
1
Table of Contents
Background................................................................................................................................3
Case study Information..............................................................................................................3
Subjective history (initial assessment)...................................................................................3
Objective history (findings)...................................................................................................4
Planter plate Tear.......................................................................................................................4
Grading.......................................................................................................................................5
Epidemiology.............................................................................................................................5
Risk factors.................................................................................................................................6
Differential diagnosis.................................................................................................................6
Assessment.................................................................................................................................7
Physical examination.............................................................................................................7
Lachmans Test.......................................................................................................................8
Scoring system for Lachman’s test....................................................................................8
Imaging..................................................................................................................................9
Management or intervention in planter plate tear......................................................................9
Non operative Interventions...................................................................................................9
Simple interventions.........................................................................................................10
Footwear modification.....................................................................................................10
Anti- inflammatory medicine...........................................................................................10
1
Table of Contents
Background................................................................................................................................3
Case study Information..............................................................................................................3
Subjective history (initial assessment)...................................................................................3
Objective history (findings)...................................................................................................4
Planter plate Tear.......................................................................................................................4
Grading.......................................................................................................................................5
Epidemiology.............................................................................................................................5
Risk factors.................................................................................................................................6
Differential diagnosis.................................................................................................................6
Assessment.................................................................................................................................7
Physical examination.............................................................................................................7
Lachmans Test.......................................................................................................................8
Scoring system for Lachman’s test....................................................................................8
Imaging..................................................................................................................................9
Management or intervention in planter plate tear......................................................................9
Non operative Interventions...................................................................................................9
Simple interventions.........................................................................................................10
Footwear modification.....................................................................................................10
Anti- inflammatory medicine...........................................................................................10
CASE STUDY ON PATHOPHYSIOLOGY
2
Stretching/ strengthening.................................................................................................10
Icing..................................................................................................................................10
Orthoses............................................................................................................................11
Operative management.........................................................................................................11
Plantar plate tear surgery..................................................................................................11
Surgery assisted in earlier problem..................................................................................11
Chronic surgery to treat plantar plate...............................................................................11
Health outcome measure..........................................................................................................12
Foot and Ankle Ability Measure..........................................................................................12
Pain examination..................................................................................................................12
References................................................................................................................................13
2
Stretching/ strengthening.................................................................................................10
Icing..................................................................................................................................10
Orthoses............................................................................................................................11
Operative management.........................................................................................................11
Plantar plate tear surgery..................................................................................................11
Surgery assisted in earlier problem..................................................................................11
Chronic surgery to treat plantar plate...............................................................................11
Health outcome measure..........................................................................................................12
Foot and Ankle Ability Measure..........................................................................................12
Pain examination..................................................................................................................12
References................................................................................................................................13
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
CASE STUDY ON PATHOPHYSIOLOGY
3
Case study on Pathophysiology
Background
The symptoms reported in the case study indicates that the patients is suffering from
Plantar plate Tearing. Planter plate tear is a common problem occurred in forefoot and can be
associated with Neuroma. This can be occurred due to lack of attention (Baravarian,
Thomson, Nazarian, 2011). The injuries occurred in foot area can be considered as damage of
supporting ligament of a toe. It includes inflammation, reduction of strength in that particular
area, and rupture, Crossover in second most toe deformation. Women are older than 50 years
affected more by plantar plate tear. This can be caused by excessive pressure on second
metatarsal by using footwear like high heeled shoes which caused peak pressure on second
most metatarsal, footwear like flocks caused excessive sweat which causes skin infection.
Sometimes, patient feels tearing sensation and feel like walking on stones. Plantar plate is a
ligament like structure provides strength to joints of metatarsal when there is excessive
pressure occurred on that area it results plantar plate tearing and further caused low stability
and dysfunction in planter plate (Camasta, 2015). It can be diagnosed by analysing symptoms
like pain and instability occurred in metatarsal area, swelling on metatarsophalangeal joints
and skin infection. Some physical diagnosis methods can be used are: X-rays, MRI
Case study Information
Subjective history (initial assessment)
The initial information provided in case study stated that the patient is a theatre nurse
Suffering from burning pain in left second metatarsal region from 12 weeks.
She is an old age women with body mass index of 28 kg/m2.
Goes to gym three times per week and wears clogs for work.
3
Case study on Pathophysiology
Background
The symptoms reported in the case study indicates that the patients is suffering from
Plantar plate Tearing. Planter plate tear is a common problem occurred in forefoot and can be
associated with Neuroma. This can be occurred due to lack of attention (Baravarian,
Thomson, Nazarian, 2011). The injuries occurred in foot area can be considered as damage of
supporting ligament of a toe. It includes inflammation, reduction of strength in that particular
area, and rupture, Crossover in second most toe deformation. Women are older than 50 years
affected more by plantar plate tear. This can be caused by excessive pressure on second
metatarsal by using footwear like high heeled shoes which caused peak pressure on second
most metatarsal, footwear like flocks caused excessive sweat which causes skin infection.
Sometimes, patient feels tearing sensation and feel like walking on stones. Plantar plate is a
ligament like structure provides strength to joints of metatarsal when there is excessive
pressure occurred on that area it results plantar plate tearing and further caused low stability
and dysfunction in planter plate (Camasta, 2015). It can be diagnosed by analysing symptoms
like pain and instability occurred in metatarsal area, swelling on metatarsophalangeal joints
and skin infection. Some physical diagnosis methods can be used are: X-rays, MRI
Case study Information
Subjective history (initial assessment)
The initial information provided in case study stated that the patient is a theatre nurse
Suffering from burning pain in left second metatarsal region from 12 weeks.
She is an old age women with body mass index of 28 kg/m2.
Goes to gym three times per week and wears clogs for work.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
CASE STUDY ON PATHOPHYSIOLOGY
4
Reported to feel pain every day after work and stated that it feels like walking in
stones.
Used to do gardening in free time.
Has a history of HAV and Diabetes type two.
She is taking Metformin medicine to control BGL.
No vascular complication.
Having no pain in first metatarsophalangeal joints. The picture of left foot of patient
showed inflammation near first toe, dislocation of second toe towards first toe and
skin infection can be seen.
Objective history (findings)
Most of the symptoms that are reported in initial case study are similar as symptoms
occur in plantar plate tear.
Faulty structure of foot like hammertoe is examined in picture
Swelling in left foot near first toe which is also called bunion
Second toe is floating and little bit upward.
First toe is leaning toward second toe
Fungal infection and calluses can be seen on base of the foot.
Swelling on the base of foot and because of this toe is floating
Planter plate Tear
Plantar plate is the disruption of plantar plate of foot occurs at distal lateral border of
the plantar plate. A plantar plate is a ligament that is situated on the underside of the
metatarsal phalangeal joints ay the ball of the foot (Pogo Physio, 2017). It is mostly occurs in
women’s of middle age and causing persistent pain and swelling in that area. It is associated
4
Reported to feel pain every day after work and stated that it feels like walking in
stones.
Used to do gardening in free time.
Has a history of HAV and Diabetes type two.
She is taking Metformin medicine to control BGL.
No vascular complication.
Having no pain in first metatarsophalangeal joints. The picture of left foot of patient
showed inflammation near first toe, dislocation of second toe towards first toe and
skin infection can be seen.
Objective history (findings)
Most of the symptoms that are reported in initial case study are similar as symptoms
occur in plantar plate tear.
Faulty structure of foot like hammertoe is examined in picture
Swelling in left foot near first toe which is also called bunion
Second toe is floating and little bit upward.
First toe is leaning toward second toe
Fungal infection and calluses can be seen on base of the foot.
Swelling on the base of foot and because of this toe is floating
Planter plate Tear
Plantar plate is the disruption of plantar plate of foot occurs at distal lateral border of
the plantar plate. A plantar plate is a ligament that is situated on the underside of the
metatarsal phalangeal joints ay the ball of the foot (Pogo Physio, 2017). It is mostly occurs in
women’s of middle age and causing persistent pain and swelling in that area. It is associated
CASE STUDY ON PATHOPHYSIOLOGY
5
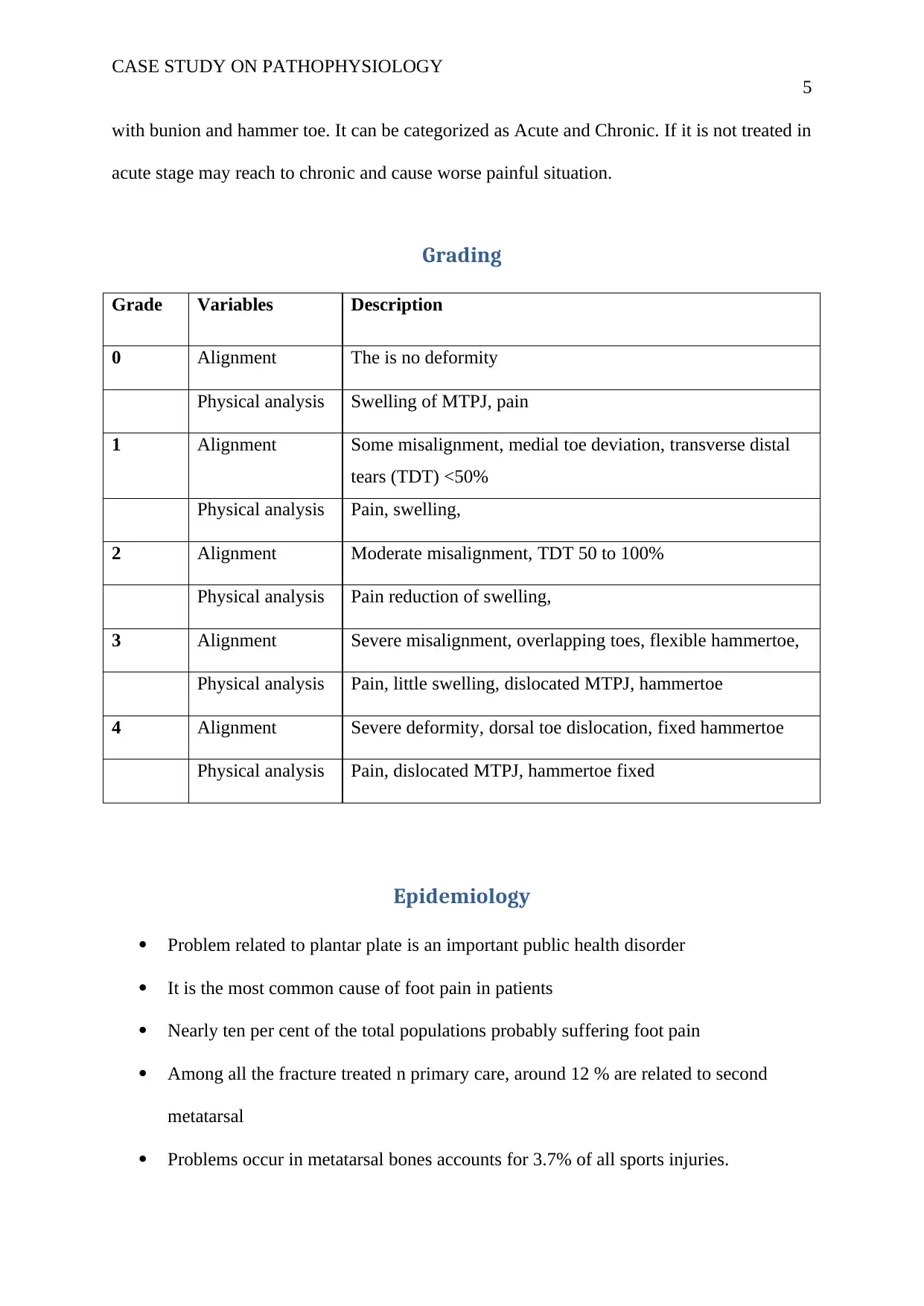
with bunion and hammer toe. It can be categorized as Acute and Chronic. If it is not treated in
acute stage may reach to chronic and cause worse painful situation.
Grading
Grade Variables Description
0 Alignment The is no deformity
Physical analysis Swelling of MTPJ, pain
1 Alignment Some misalignment, medial toe deviation, transverse distal
tears (TDT) <50%
Physical analysis Pain, swelling,
2 Alignment Moderate misalignment, TDT 50 to 100%
Physical analysis Pain reduction of swelling,
3 Alignment Severe misalignment, overlapping toes, flexible hammertoe,
Physical analysis Pain, little swelling, dislocated MTPJ, hammertoe
4 Alignment Severe deformity, dorsal toe dislocation, fixed hammertoe
Physical analysis Pain, dislocated MTPJ, hammertoe fixed
Epidemiology
Problem related to plantar plate is an important public health disorder
It is the most common cause of foot pain in patients
Nearly ten per cent of the total populations probably suffering foot pain
Among all the fracture treated n primary care, around 12 % are related to second
metatarsal
Problems occur in metatarsal bones accounts for 3.7% of all sports injuries.
5
with bunion and hammer toe. It can be categorized as Acute and Chronic. If it is not treated in
acute stage may reach to chronic and cause worse painful situation.
Grading
Grade Variables Description
0 Alignment The is no deformity
Physical analysis Swelling of MTPJ, pain
1 Alignment Some misalignment, medial toe deviation, transverse distal
tears (TDT) <50%
Physical analysis Pain, swelling,
2 Alignment Moderate misalignment, TDT 50 to 100%
Physical analysis Pain reduction of swelling,
3 Alignment Severe misalignment, overlapping toes, flexible hammertoe,
Physical analysis Pain, little swelling, dislocated MTPJ, hammertoe
4 Alignment Severe deformity, dorsal toe dislocation, fixed hammertoe
Physical analysis Pain, dislocated MTPJ, hammertoe fixed
Epidemiology
Problem related to plantar plate is an important public health disorder
It is the most common cause of foot pain in patients
Nearly ten per cent of the total populations probably suffering foot pain
Among all the fracture treated n primary care, around 12 % are related to second
metatarsal
Problems occur in metatarsal bones accounts for 3.7% of all sports injuries.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
CASE STUDY ON PATHOPHYSIOLOGY
6
Around 20% athletes suffered with metatarsal injuries once in a life.
The second toe deformity was originally described in 1987.since than great number of
patients has been diagnosed with this faulty foot problem.
Risk factors
Age
Sex
BMI
WEIGHT
Footwear
Unusual Walk Or Foot Position
Heavy Weight Exercises
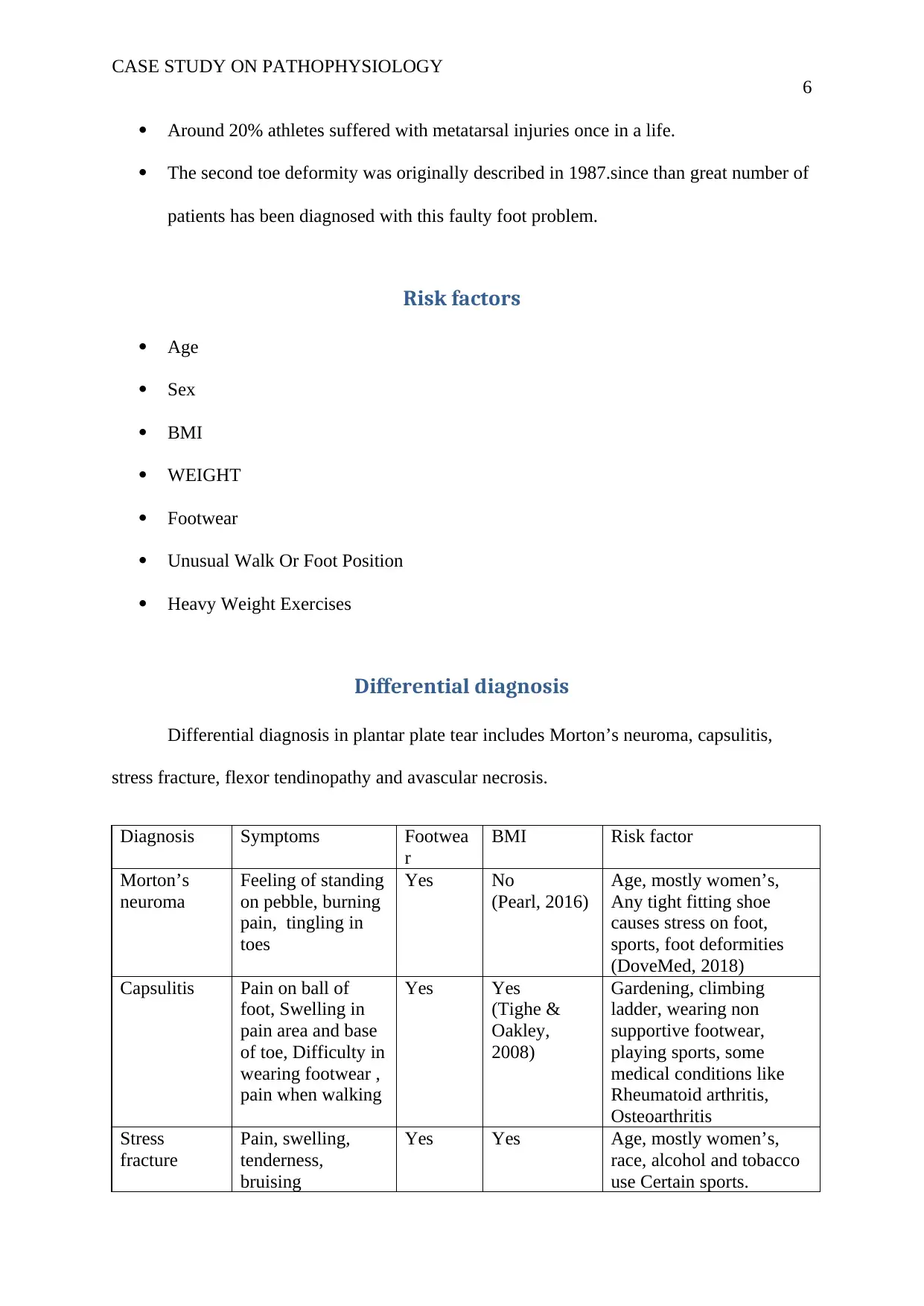
Differential diagnosis
Differential diagnosis in plantar plate tear includes Morton’s neuroma, capsulitis,
stress fracture, flexor tendinopathy and avascular necrosis.
Diagnosis Symptoms Footwea
r
BMI Risk factor
Morton’s
neuroma
Feeling of standing
on pebble, burning
pain, tingling in
toes
Yes No
(Pearl, 2016)
Age, mostly women’s,
Any tight fitting shoe
causes stress on foot,
sports, foot deformities
(DoveMed, 2018)
Capsulitis Pain on ball of
foot, Swelling in
pain area and base
of toe, Difficulty in
wearing footwear ,
pain when walking
Yes Yes
(Tighe &
Oakley,
2008)
Gardening, climbing
ladder, wearing non
supportive footwear,
playing sports, some
medical conditions like
Rheumatoid arthritis,
Osteoarthritis
Stress
fracture
Pain, swelling,
tenderness,
bruising
Yes Yes Age, mostly women’s,
race, alcohol and tobacco
use Certain sports.
6
Around 20% athletes suffered with metatarsal injuries once in a life.
The second toe deformity was originally described in 1987.since than great number of
patients has been diagnosed with this faulty foot problem.
Risk factors
Age
Sex
BMI
WEIGHT
Footwear
Unusual Walk Or Foot Position
Heavy Weight Exercises
Differential diagnosis
Differential diagnosis in plantar plate tear includes Morton’s neuroma, capsulitis,
stress fracture, flexor tendinopathy and avascular necrosis.
Diagnosis Symptoms Footwea
r
BMI Risk factor
Morton’s
neuroma
Feeling of standing
on pebble, burning
pain, tingling in
toes
Yes No
(Pearl, 2016)
Age, mostly women’s,
Any tight fitting shoe
causes stress on foot,
sports, foot deformities
(DoveMed, 2018)
Capsulitis Pain on ball of
foot, Swelling in
pain area and base
of toe, Difficulty in
wearing footwear ,
pain when walking
Yes Yes
(Tighe &
Oakley,
2008)
Gardening, climbing
ladder, wearing non
supportive footwear,
playing sports, some
medical conditions like
Rheumatoid arthritis,
Osteoarthritis
Stress
fracture
Pain, swelling,
tenderness,
bruising
Yes Yes Age, mostly women’s,
race, alcohol and tobacco
use Certain sports.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
CASE STUDY ON PATHOPHYSIOLOGY
7
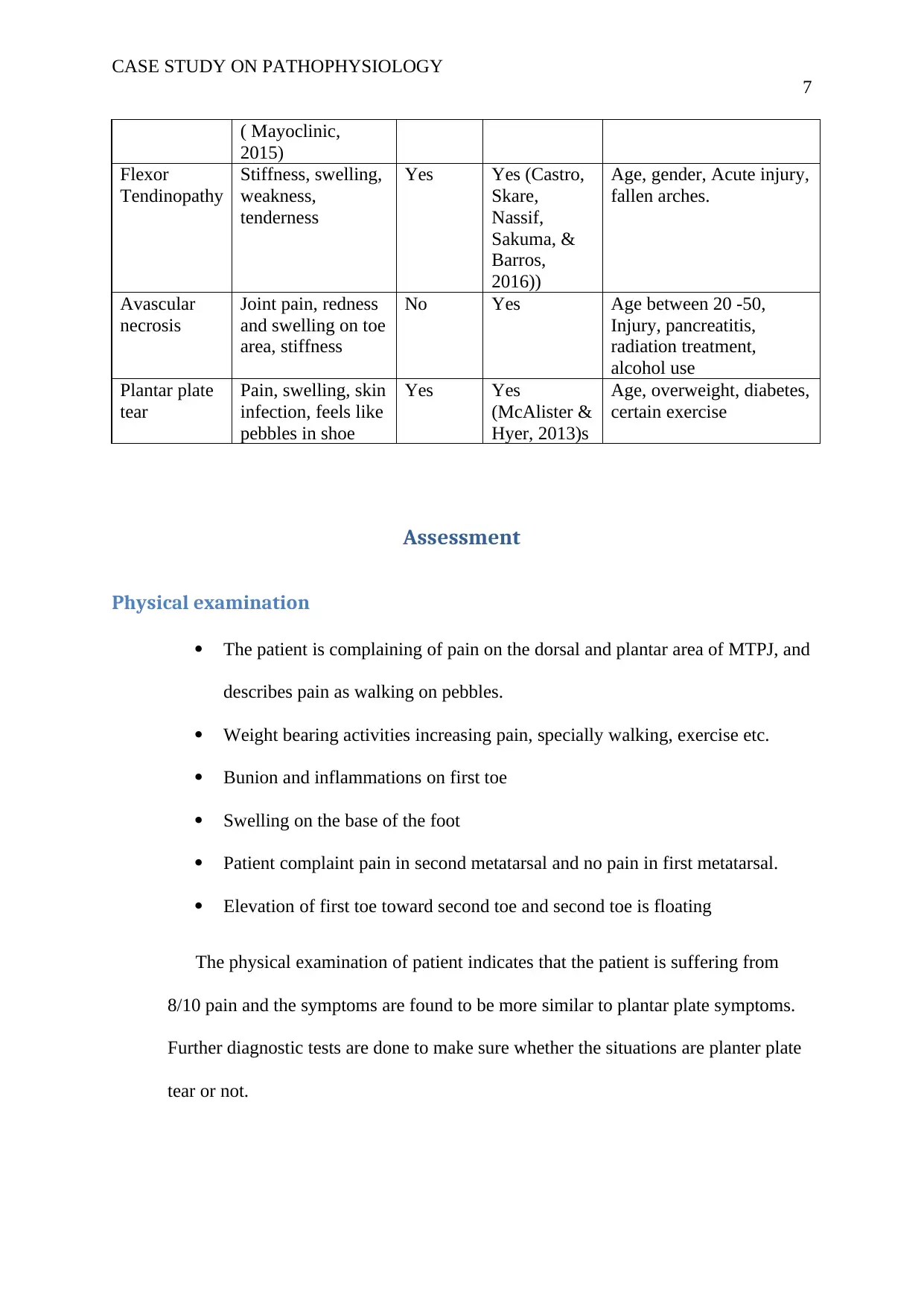
( Mayoclinic,
2015)
Flexor
Tendinopathy
Stiffness, swelling,
weakness,
tenderness
Yes Yes (Castro,
Skare,
Nassif,
Sakuma, &
Barros,
2016))
Age, gender, Acute injury,
fallen arches.
Avascular
necrosis
Joint pain, redness
and swelling on toe
area, stiffness
No Yes Age between 20 -50,
Injury, pancreatitis,
radiation treatment,
alcohol use
Plantar plate
tear
Pain, swelling, skin
infection, feels like
pebbles in shoe
Yes Yes
(McAlister &
Hyer, 2013)s
Age, overweight, diabetes,
certain exercise
Assessment
Physical examination
The patient is complaining of pain on the dorsal and plantar area of MTPJ, and
describes pain as walking on pebbles.
Weight bearing activities increasing pain, specially walking, exercise etc.
Bunion and inflammations on first toe
Swelling on the base of the foot
Patient complaint pain in second metatarsal and no pain in first metatarsal.
Elevation of first toe toward second toe and second toe is floating
The physical examination of patient indicates that the patient is suffering from
8/10 pain and the symptoms are found to be more similar to plantar plate symptoms.
Further diagnostic tests are done to make sure whether the situations are planter plate
tear or not.
7
( Mayoclinic,
2015)
Flexor
Tendinopathy
Stiffness, swelling,
weakness,
tenderness
Yes Yes (Castro,
Skare,
Nassif,
Sakuma, &
Barros,
2016))
Age, gender, Acute injury,
fallen arches.
Avascular
necrosis
Joint pain, redness
and swelling on toe
area, stiffness
No Yes Age between 20 -50,
Injury, pancreatitis,
radiation treatment,
alcohol use
Plantar plate
tear
Pain, swelling, skin
infection, feels like
pebbles in shoe
Yes Yes
(McAlister &
Hyer, 2013)s
Age, overweight, diabetes,
certain exercise
Assessment
Physical examination
The patient is complaining of pain on the dorsal and plantar area of MTPJ, and
describes pain as walking on pebbles.
Weight bearing activities increasing pain, specially walking, exercise etc.
Bunion and inflammations on first toe
Swelling on the base of the foot
Patient complaint pain in second metatarsal and no pain in first metatarsal.
Elevation of first toe toward second toe and second toe is floating
The physical examination of patient indicates that the patient is suffering from
8/10 pain and the symptoms are found to be more similar to plantar plate symptoms.
Further diagnostic tests are done to make sure whether the situations are planter plate
tear or not.
CASE STUDY ON PATHOPHYSIOLOGY
8
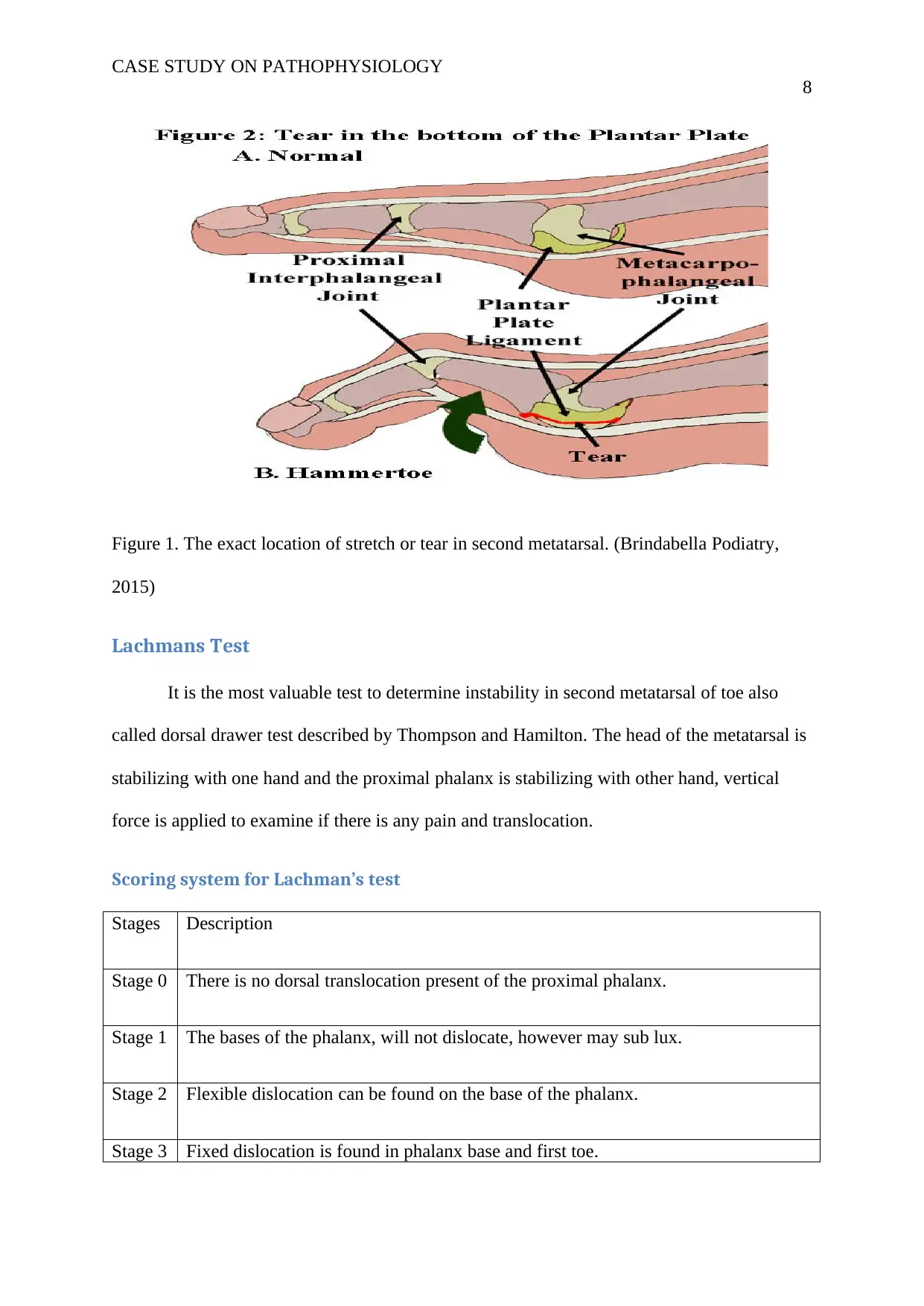
Figure 1. The exact location of stretch or tear in second metatarsal. (Brindabella Podiatry,
2015)
Lachmans Test
It is the most valuable test to determine instability in second metatarsal of toe also
called dorsal drawer test described by Thompson and Hamilton. The head of the metatarsal is
stabilizing with one hand and the proximal phalanx is stabilizing with other hand, vertical
force is applied to examine if there is any pain and translocation.
Scoring system for Lachman’s test
Stages Description
Stage 0 There is no dorsal translocation present of the proximal phalanx.
Stage 1 The bases of the phalanx, will not dislocate, however may sub lux.
Stage 2 Flexible dislocation can be found on the base of the phalanx.
Stage 3 Fixed dislocation is found in phalanx base and first toe.
8
Figure 1. The exact location of stretch or tear in second metatarsal. (Brindabella Podiatry,
2015)
Lachmans Test
It is the most valuable test to determine instability in second metatarsal of toe also
called dorsal drawer test described by Thompson and Hamilton. The head of the metatarsal is
stabilizing with one hand and the proximal phalanx is stabilizing with other hand, vertical
force is applied to examine if there is any pain and translocation.
Scoring system for Lachman’s test
Stages Description
Stage 0 There is no dorsal translocation present of the proximal phalanx.
Stage 1 The bases of the phalanx, will not dislocate, however may sub lux.
Stage 2 Flexible dislocation can be found on the base of the phalanx.
Stage 3 Fixed dislocation is found in phalanx base and first toe.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
CASE STUDY ON PATHOPHYSIOLOGY
9
Result - The patient is diagnosed with stage 3.
Imaging
Arthrogram and MRI is used to diagnose plantar plate tear. Arhtogram is very helpful
to determine the integrity of the ligament structure surrounding the joint. A needle is injected
into the joints and radiography dye is injected to see if any fluid leaks out. MRI of foot allows
direct visualization of plantar plate. Joint alignment is viewed by using x rays.
Radiographic criteria for instability
Lack of concentration of joint.
Lateral or medial deviation of proximal phalanx >5 degree.
Clawing on lateral radiograph.
Patient is also gone through MRI and Arhtogram test of second MTPJ. Plantar plate and
collateral ligament tears diagnosed.
Management or intervention in planter plate tear
Planter plate tear can be diagnosed by analysing the symptoms and complications
occurred in foot are, by X-rays, magnetic resonance imaging (MRI) and arthrogram.
Non operative Interventions
Divide according to the type of injury. Like acute and chronic injury. Acute injury is
examined by surgeon to determine if surgery is necessary or not. If the surgery is not
9
Result - The patient is diagnosed with stage 3.
Imaging
Arthrogram and MRI is used to diagnose plantar plate tear. Arhtogram is very helpful
to determine the integrity of the ligament structure surrounding the joint. A needle is injected
into the joints and radiography dye is injected to see if any fluid leaks out. MRI of foot allows
direct visualization of plantar plate. Joint alignment is viewed by using x rays.
Radiographic criteria for instability
Lack of concentration of joint.
Lateral or medial deviation of proximal phalanx >5 degree.
Clawing on lateral radiograph.
Patient is also gone through MRI and Arhtogram test of second MTPJ. Plantar plate and
collateral ligament tears diagnosed.
Management or intervention in planter plate tear
Planter plate tear can be diagnosed by analysing the symptoms and complications
occurred in foot are, by X-rays, magnetic resonance imaging (MRI) and arthrogram.
Non operative Interventions
Divide according to the type of injury. Like acute and chronic injury. Acute injury is
examined by surgeon to determine if surgery is necessary or not. If the surgery is not
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
CASE STUDY ON PATHOPHYSIOLOGY
10
essential than the toe will be taped and splinted to get it heal. Some of the cases required
casting and crutches if the symptoms occurred more than 8 weeks before.
Simple interventions
wear footwear that are supportive to the foot , avoid using high heels
arch support will be effective
shoes with wide toe box should be used
periodic callus care should be considered
Footwear modification
Footwear like high heels and flexible minimalist shoes tends to increase risk of
plantar plate injury. Some of the other footwear like open toe shoe and flip flops also
associated with this problem. Risk of developing the problem will be reduces after using
recommended shoes, the patients is using clogs that are causing skin infection on foot. By
avowing these shoes the infection will also be reduced. According to Moore (2018) a long,
softer shoe can reduce the direct and indirect stress on second metatarsal.
Anti- inflammatory medicine
As patient reports inflammation on the first toe area it is essential to reduce it for
relief. Anti-inflammatory like aspirin, ibuprofen and naproxen will be prescribed in this case.
Anti-inflammatory medicines are helpful to decrease the inflammation and relief pain in
affected area (Frank, 2015).
Stretching/ strengthening
Applying stretching on foot muscle that are tight and lack of strength. To provide
strength and flexibility to the muscles. Daily strengthening and stretching workouts helps to
treat plantar plate tear (Bishop, 2017).
10
essential than the toe will be taped and splinted to get it heal. Some of the cases required
casting and crutches if the symptoms occurred more than 8 weeks before.
Simple interventions
wear footwear that are supportive to the foot , avoid using high heels
arch support will be effective
shoes with wide toe box should be used
periodic callus care should be considered
Footwear modification
Footwear like high heels and flexible minimalist shoes tends to increase risk of
plantar plate injury. Some of the other footwear like open toe shoe and flip flops also
associated with this problem. Risk of developing the problem will be reduces after using
recommended shoes, the patients is using clogs that are causing skin infection on foot. By
avowing these shoes the infection will also be reduced. According to Moore (2018) a long,
softer shoe can reduce the direct and indirect stress on second metatarsal.
Anti- inflammatory medicine
As patient reports inflammation on the first toe area it is essential to reduce it for
relief. Anti-inflammatory like aspirin, ibuprofen and naproxen will be prescribed in this case.
Anti-inflammatory medicines are helpful to decrease the inflammation and relief pain in
affected area (Frank, 2015).
Stretching/ strengthening
Applying stretching on foot muscle that are tight and lack of strength. To provide
strength and flexibility to the muscles. Daily strengthening and stretching workouts helps to
treat plantar plate tear (Bishop, 2017).
CASE STUDY ON PATHOPHYSIOLOGY
11
Icing
By applying ice directly on affected area of foot. Icing is the oldest methods to treat
musculoskeletal injuries. It can reduce inflammation, swelling and pain (Camasta, 2015).
Orthoses
It is an artificial external device used to support foot; a metatarsal dome is proximal to
the second metatarsal head with extension and cur out around the MTPJ area. It is helpful to
offload plantar plate while walking (Goom, 2017).
Operative management
Most of the injuries treat through no operative methods it not treated with these
methods than surgeries applied to them are for instant relief form the painful situation there
are two types of surgeries:
Plantar plate tear surgery
In this method the surgery is applied to the affected area to repair plantar plate tear. It
directly treats or repair plantar plate. It is totally depends on time of injury reason of tear and
the physical structure of the foot
Surgery assisted in earlier problem
This is also called primary repair to the metatarsal and it is done by directly apply a
cut on the skin and the displaced parts treated, is some of the cases plastic surgery is applied.
Chronic surgery to treat plantar plate
Planter plate tear needed to be examined before doing chronic surgery it is also called
secondary surgery. It is applied in chronic cases where the pain is not treated with primary
treatments. It is especially assisted in the case of dislocated toe or hammer toe.
11
Icing
By applying ice directly on affected area of foot. Icing is the oldest methods to treat
musculoskeletal injuries. It can reduce inflammation, swelling and pain (Camasta, 2015).
Orthoses
It is an artificial external device used to support foot; a metatarsal dome is proximal to
the second metatarsal head with extension and cur out around the MTPJ area. It is helpful to
offload plantar plate while walking (Goom, 2017).
Operative management
Most of the injuries treat through no operative methods it not treated with these
methods than surgeries applied to them are for instant relief form the painful situation there
are two types of surgeries:
Plantar plate tear surgery
In this method the surgery is applied to the affected area to repair plantar plate tear. It
directly treats or repair plantar plate. It is totally depends on time of injury reason of tear and
the physical structure of the foot
Surgery assisted in earlier problem
This is also called primary repair to the metatarsal and it is done by directly apply a
cut on the skin and the displaced parts treated, is some of the cases plastic surgery is applied.
Chronic surgery to treat plantar plate
Planter plate tear needed to be examined before doing chronic surgery it is also called
secondary surgery. It is applied in chronic cases where the pain is not treated with primary
treatments. It is especially assisted in the case of dislocated toe or hammer toe.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 15



Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.