HLTAAP003: Pneumonia Case Study Analysis, Treatment and Care Plan
VerifiedAdded on 2023/06/04
|8
|1716
|315
Case Study
AI Summary
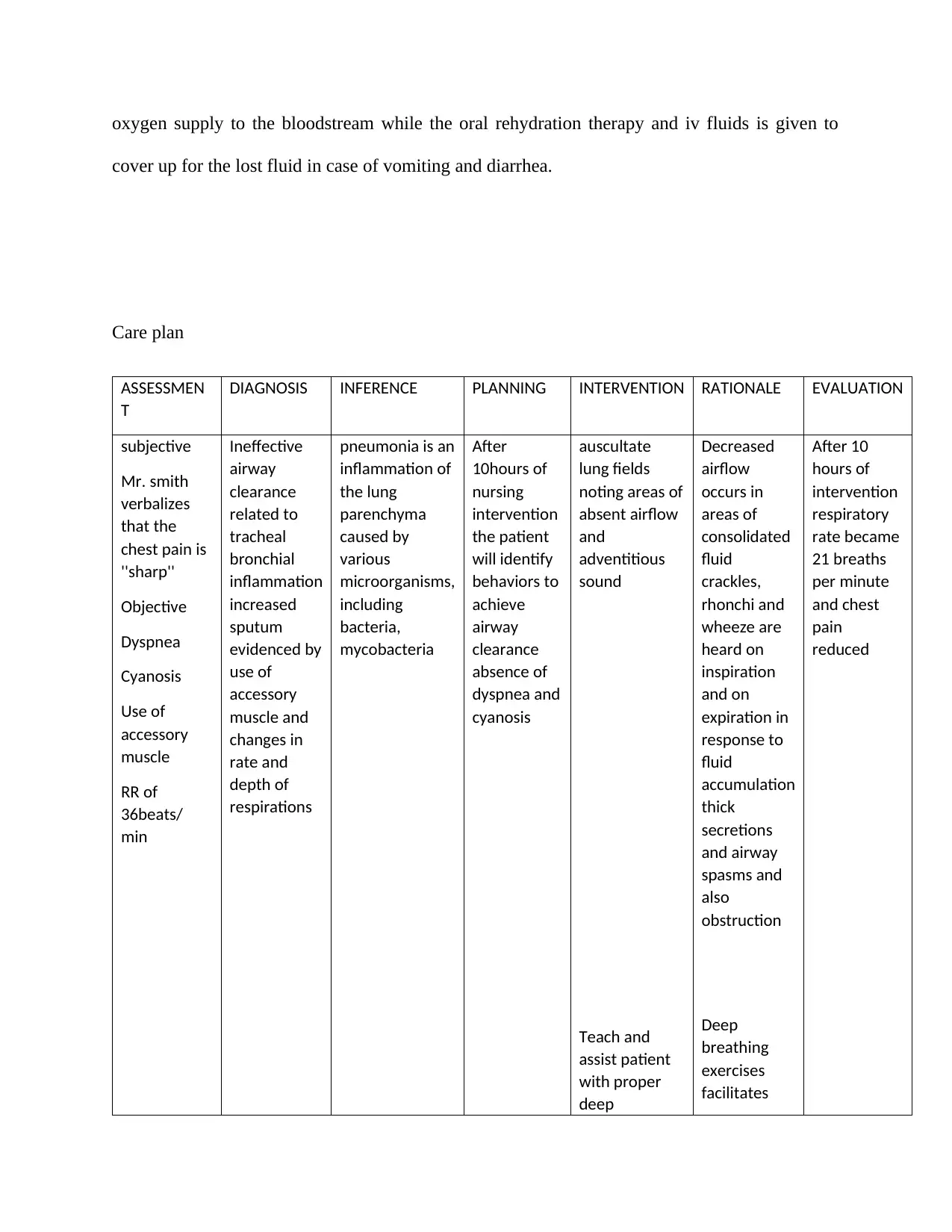
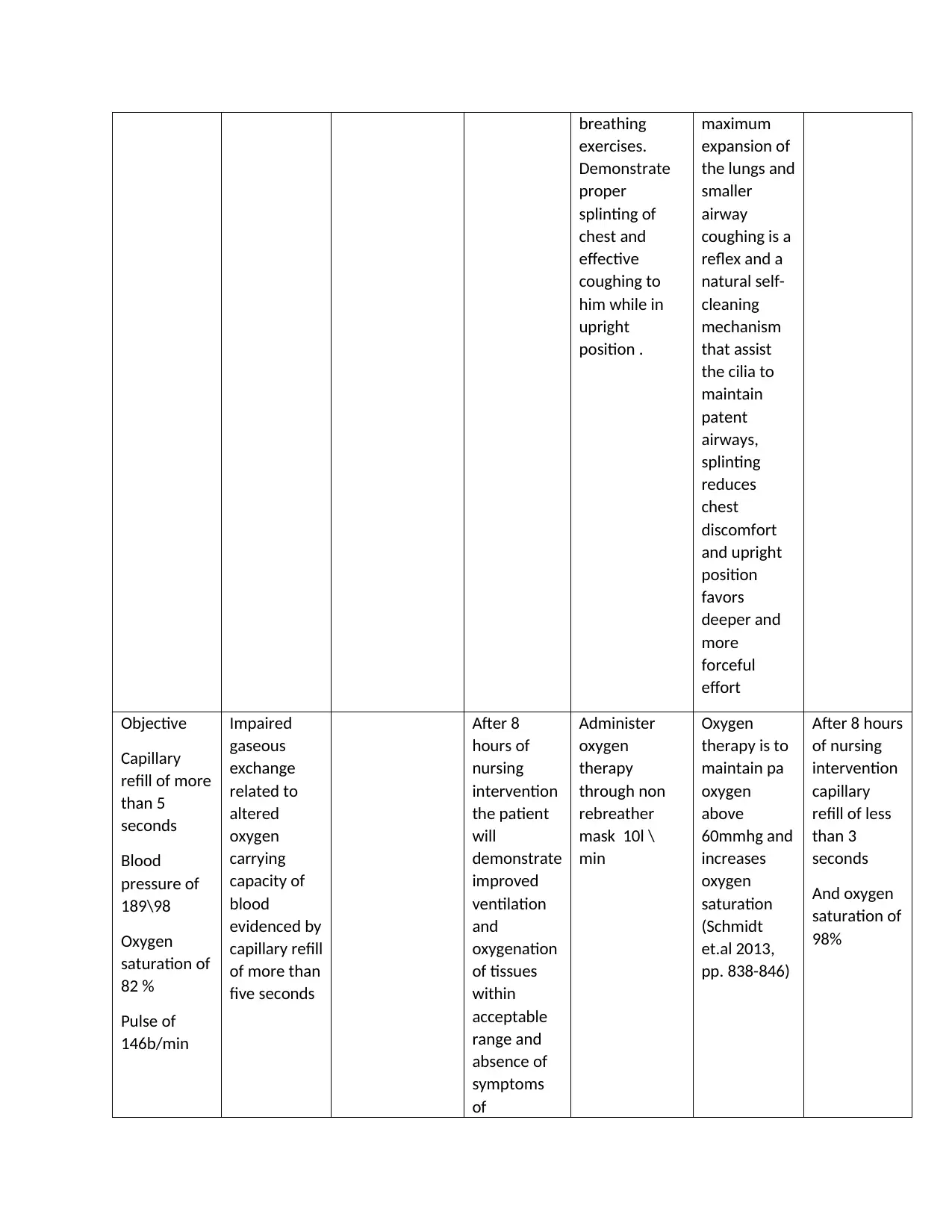
This case study examines a patient diagnosed with pneumonia, focusing on the analysis of the patient's symptoms, vital signs, and medical history, including diabetes and bronchitis. The document delves into the pathophysiology of pneumonia, explaining how the infection affects the lungs and triggers an immune response. It analyzes the significance of the patient's elevated respiratory rate, fever, and low oxygen saturation, relating them to the disease process. The case study also explores the patient's history of diabetes and its impact on their susceptibility to infection. Furthermore, it outlines potential treatment options, including antibiotics and supportive care such as oxygen therapy and intravenous fluids, and proposes a comprehensive nursing care plan. The care plan details assessment, diagnosis, planning, intervention, rationale, and evaluation, providing a structured approach to managing the patient's condition and promoting improved ventilation and oxygenation.


1 out of 8
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.