Reflective Practice Model: Gibbs' Reflective Cycle
This assignment requires the student to reflect on and improve their own clinical practice through a case study. The student must provide satisfactory answers to the related questions using reliable sources and proper referencing.
7 Pages2606 Words406 Views
Added on 2023-04-21
About This Document
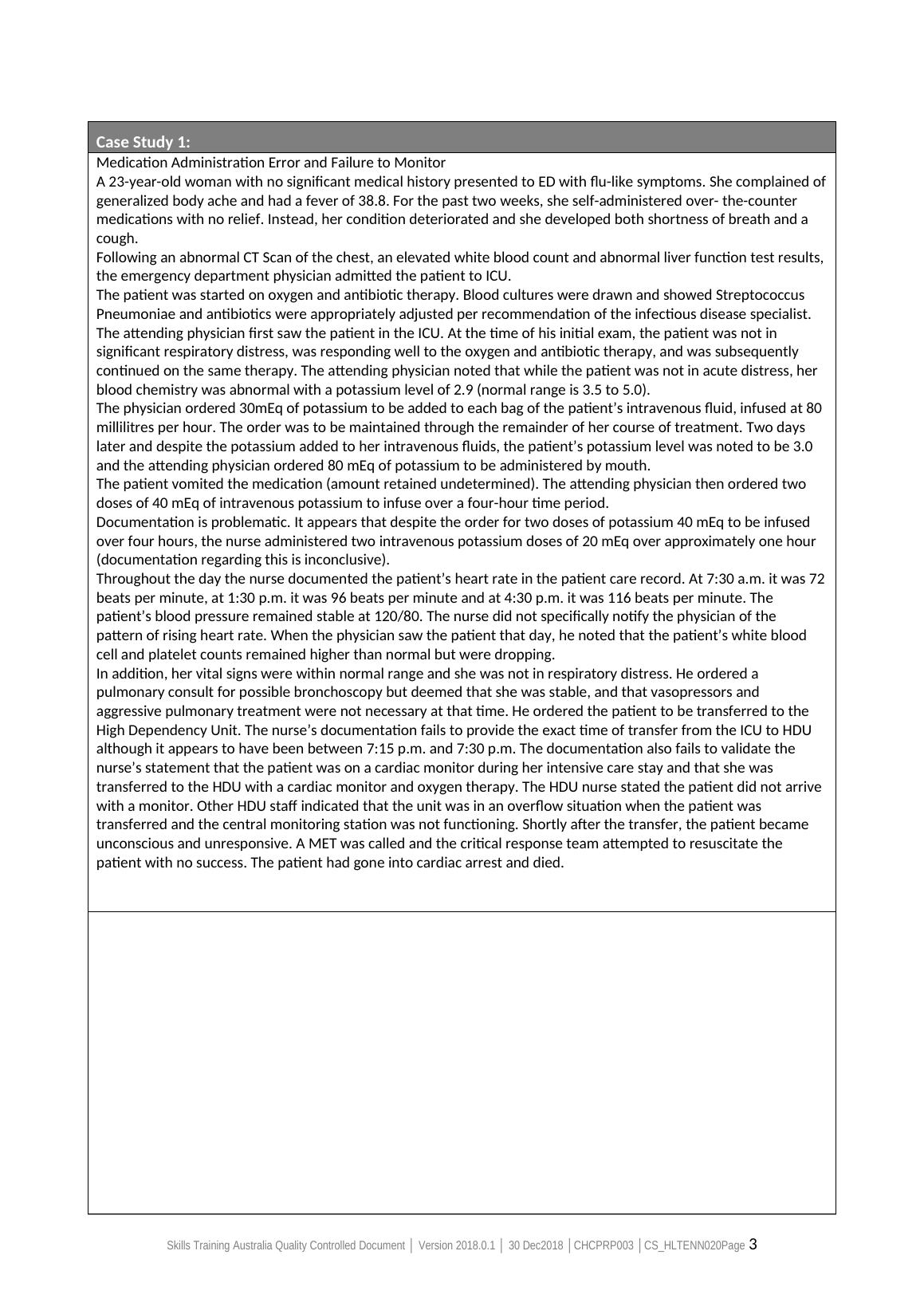
This document discusses Gibbs' Reflective Cycle, a model of reflective practice, and applies it to a case study involving a medication administration error and failure to monitor. It outlines the steps of the model and the conclusions drawn for improving practice.
Reflective Practice Model: Gibbs' Reflective Cycle
This assignment requires the student to reflect on and improve their own clinical practice through a case study. The student must provide satisfactory answers to the related questions using reliable sources and proper referencing.
Added on 2023-04-21
ShareRelated Documents
End of preview
Want to access all the pages? Upload your documents or become a member.
Reflective Practice Models: Kolb's Learning Cycle
|7
|2510
|347
Nursing Process and Intervention for Mr. Jones and Mr. Smith
|14
|6012
|409
Effective Communication in Healthcare
|28
|3700
|61
Submitted entered in database
|28
|4207
|19
CHCCSM005 Develop, Facilitate and Review All Aspects of Case Management - Student Assessment Workbook
|26
|8569
|354
Unit Assessment Pack (UAP) – Cover Sheet for CHCDIS002
|23
|5741
|230