Professional Nursing Practice - PDF
VerifiedAdded on 2021/05/31
|14
|3287
|35
AI Summary
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.

Running head: PROFESSIONAL NURSING PRACTICE
PROFESSIONAL NURSING PRACTICE
Name of the Student
Name of the University
Author note
PROFESSIONAL NURSING PRACTICE
Name of the Student
Name of the University
Author note
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
1PROFESSIONAL NURSING PRACTICE
The National Safety Quality Health Service (NSQHS) standard is a set of 10 standards
that are developed by the Australian Commission on Safety and Quality in Healthcare (ACSQH).
This standard was developed with collaboration and consultation between jurisdiction service,
technical experts and the range of different stakeholders starting from health care experts to the
service users or patients (National Safety and Quality Health Service Standards. 2012). The
primary aim of the standards is to provide security to the patients from harm and enhance the
quality of Healthcare service provision. This is achieved by providing a quality assurance
mechanism that assesses the relevancy of the healthcare system and the level of compliance it
has with the NSQHS. It also helps to improve the health care facility’s mechanism by providing
them with inspirational or developmental goals (Greenfield et al., 2012). Within this 10 National
safety and quality health service standards, preventive and controlling Healthcare associated
infection or standard 3 has been chosen for the discussion. The primary aim of the standard is
to describe the Healthcare systems and their used strategies for prevention of infection within
patients in the Healthcare system and it assures that Healthcare facilities are being able to
manage infections effectively and minimise the consequences or not. Thereby the primary
intention of this standard is to protect the patients from different Healthcare associated infections
in the Healthcare facility and manage the infections with evidence-based strategies (McSherry et
al., 2012). In this assignment, a critical discussion of quality and safety in the Healthcare system
with respect to the standard three of NSQHS standard will be discussed with support from
different scholarly literature. Further, critical discussion of a clinical activity relevant to standard
three, which the risk on impact of low quality care and the strategies to manage or improve the
situation will be discussed. Finally, the process of outcome data correction, analysis and
improvements will be discussed with reference of recent literatures.
The National Safety Quality Health Service (NSQHS) standard is a set of 10 standards
that are developed by the Australian Commission on Safety and Quality in Healthcare (ACSQH).
This standard was developed with collaboration and consultation between jurisdiction service,
technical experts and the range of different stakeholders starting from health care experts to the
service users or patients (National Safety and Quality Health Service Standards. 2012). The
primary aim of the standards is to provide security to the patients from harm and enhance the
quality of Healthcare service provision. This is achieved by providing a quality assurance
mechanism that assesses the relevancy of the healthcare system and the level of compliance it
has with the NSQHS. It also helps to improve the health care facility’s mechanism by providing
them with inspirational or developmental goals (Greenfield et al., 2012). Within this 10 National
safety and quality health service standards, preventive and controlling Healthcare associated
infection or standard 3 has been chosen for the discussion. The primary aim of the standard is
to describe the Healthcare systems and their used strategies for prevention of infection within
patients in the Healthcare system and it assures that Healthcare facilities are being able to
manage infections effectively and minimise the consequences or not. Thereby the primary
intention of this standard is to protect the patients from different Healthcare associated infections
in the Healthcare facility and manage the infections with evidence-based strategies (McSherry et
al., 2012). In this assignment, a critical discussion of quality and safety in the Healthcare system
with respect to the standard three of NSQHS standard will be discussed with support from
different scholarly literature. Further, critical discussion of a clinical activity relevant to standard
three, which the risk on impact of low quality care and the strategies to manage or improve the
situation will be discussed. Finally, the process of outcome data correction, analysis and
improvements will be discussed with reference of recent literatures.
2PROFESSIONAL NURSING PRACTICE
After the creation of national safety and quality health service standards, the Healthcare
facilities are being provided with a quality assurance mechanism that helps to determine the
relevancy of the system and ensures that safety and quality standards are met (Slimings et al.,
2014). The implementation of national standards in Healthcare facilities also helps in
improvement of Patient Safety especially in case of hospital-acquired infections. The Healthcare
facilities are being pushed to monitor and take proper action against safety and quality related
issues. They are also involved in designing user-friendly quality processes so that the affected
system can be improved and continuously monitored through clinical audits and interventions
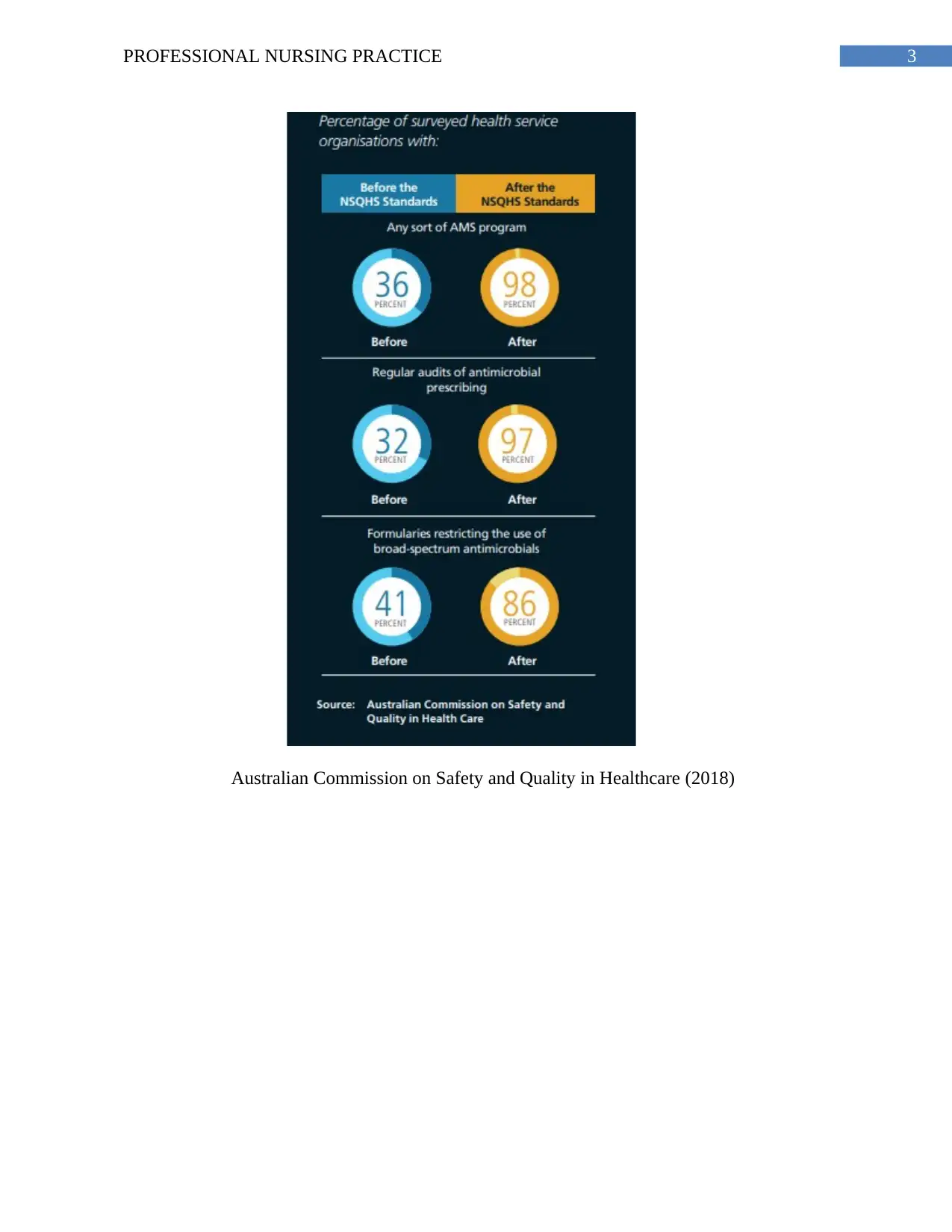
(Runciman et al., 2012). The standard 3 of NSQHS determines that 30 to 40% of hospitals in
Australia prescribed antibiotics. However, within that there are Healthcare facilities that do not
prescribe appropriate type of antibiotics, its dose and duration. Hereby, leading to resistance to
antibiotics and decreasing the patient’s ability to fight microbes or infections. Therefore, the
Healthcare facilities are using antimicrobial stewardship program (AMS) in which the use of
antimicrobials can be optimised through activities such as feedback, audits, comparing
prescribed antibiotics to peer’s, prescribing restrictions. Therefore, those Healthcare
professionals can double check the prescription before handing it over to the patients. The
Australian Bureau of statistics has determined that after the implementation of AMS, hospitals
are focused to identify the reason of long patient stays and determine the effectiveness of their
medication system (Zingg et al., 2015). Following are the data acquired from The State of Safety
and Quality in Australian Health Care (2016).
After the creation of national safety and quality health service standards, the Healthcare
facilities are being provided with a quality assurance mechanism that helps to determine the
relevancy of the system and ensures that safety and quality standards are met (Slimings et al.,
2014). The implementation of national standards in Healthcare facilities also helps in
improvement of Patient Safety especially in case of hospital-acquired infections. The Healthcare
facilities are being pushed to monitor and take proper action against safety and quality related
issues. They are also involved in designing user-friendly quality processes so that the affected
system can be improved and continuously monitored through clinical audits and interventions
(Runciman et al., 2012). The standard 3 of NSQHS determines that 30 to 40% of hospitals in
Australia prescribed antibiotics. However, within that there are Healthcare facilities that do not
prescribe appropriate type of antibiotics, its dose and duration. Hereby, leading to resistance to
antibiotics and decreasing the patient’s ability to fight microbes or infections. Therefore, the
Healthcare facilities are using antimicrobial stewardship program (AMS) in which the use of
antimicrobials can be optimised through activities such as feedback, audits, comparing
prescribed antibiotics to peer’s, prescribing restrictions. Therefore, those Healthcare
professionals can double check the prescription before handing it over to the patients. The
Australian Bureau of statistics has determined that after the implementation of AMS, hospitals
are focused to identify the reason of long patient stays and determine the effectiveness of their
medication system (Zingg et al., 2015). Following are the data acquired from The State of Safety
and Quality in Australian Health Care (2016).
3PROFESSIONAL NURSING PRACTICE
Australian Commission on Safety and Quality in Healthcare (2018)
Australian Commission on Safety and Quality in Healthcare (2018)
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
4PROFESSIONAL NURSING PRACTICE
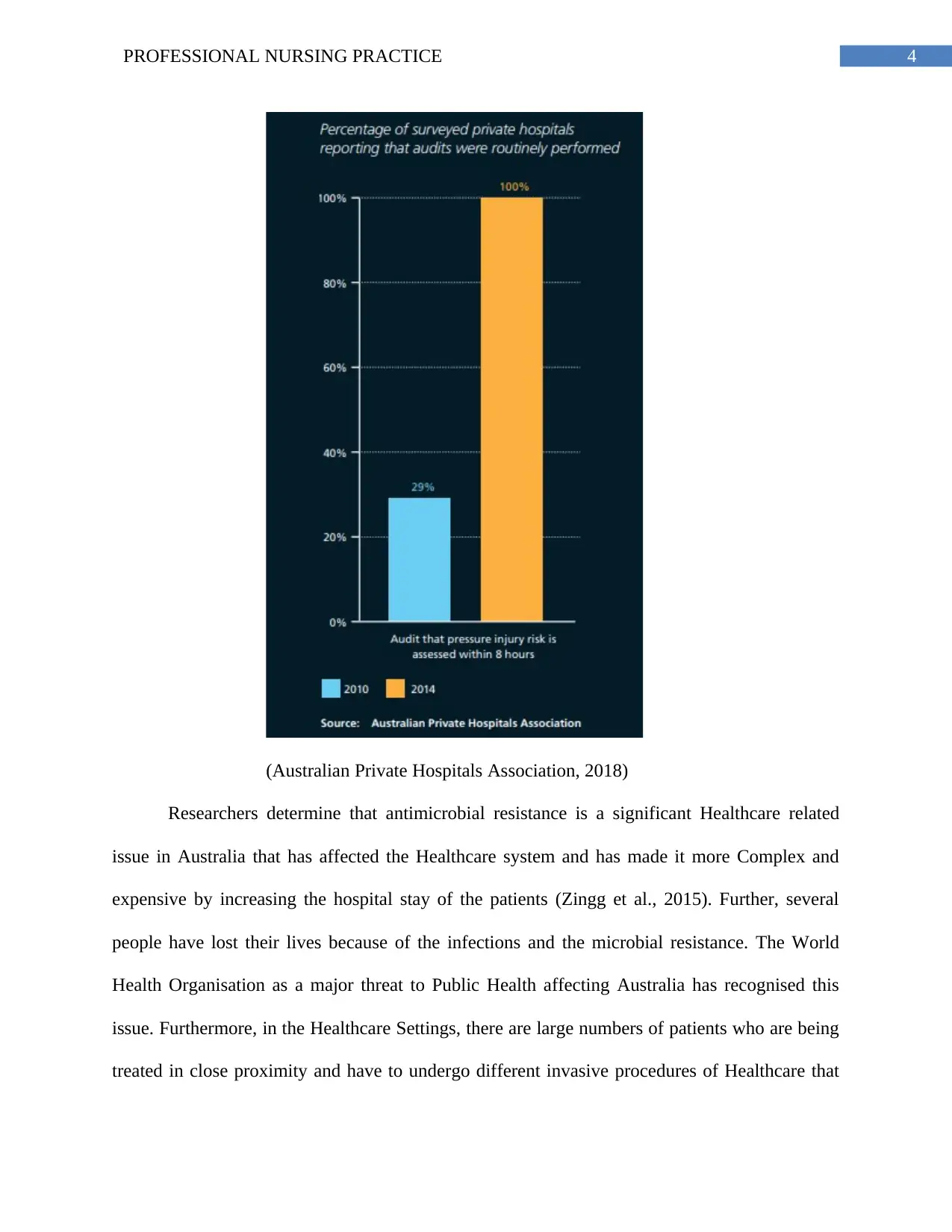
(Australian Private Hospitals Association, 2018)
Researchers determine that antimicrobial resistance is a significant Healthcare related
issue in Australia that has affected the Healthcare system and has made it more Complex and
expensive by increasing the hospital stay of the patients (Zingg et al., 2015). Further, several
people have lost their lives because of the infections and the microbial resistance. The World
Health Organisation as a major threat to Public Health affecting Australia has recognised this
issue. Furthermore, in the Healthcare Settings, there are large numbers of patients who are being
treated in close proximity and have to undergo different invasive procedures of Healthcare that
(Australian Private Hospitals Association, 2018)
Researchers determine that antimicrobial resistance is a significant Healthcare related
issue in Australia that has affected the Healthcare system and has made it more Complex and
expensive by increasing the hospital stay of the patients (Zingg et al., 2015). Further, several
people have lost their lives because of the infections and the microbial resistance. The World
Health Organisation as a major threat to Public Health affecting Australia has recognised this
issue. Furthermore, in the Healthcare Settings, there are large numbers of patients who are being
treated in close proximity and have to undergo different invasive procedures of Healthcare that
5PROFESSIONAL NURSING PRACTICE
provides an opportunity to the pathogen to adapt and spread within a number of individuals.
Hence, each year Healthcare associated infections are recorded in a large number of patients
making it as the most common concern of hospitals (Cimiotti et al., 2012). However, it has been
seen that majority of the Healthcare associated infections are preventable and researchers believe
that there are mechanism through which these Hospital acquired infections can be minimised.
Successful infection control strategy requires cumulative effort of all the approaches such as
infection control hygienic surveillance safe and appropriate use of antibiotics and antimicrobial
stewardship (Magill et al., 2014).
While discussing the risk of clinical care activity related to standard 3 the impact of low
quality care and process to improve it should be discussed. Several strategies have been
mentioned to prevent and control the Healthcare associated infection, which are being developed
and implemented by Healthcare facilities in Australia. The first risk associated with effective
governance and management system for Healthcare associated infection. Laxminarayan et al.,
(2013) determine that developing and implementation of effective governance system for
infection prevention and control can help to decrease the risk of Healthcare associated infections
in patients. To achieve this, several approaches that can be taken and implemented as policy or
procedures such as using different aseptic techniques, using the standard related to infection
control, proper processing of reusable medical devices, cleaning and maintaining an adequate
environment through disinfection. Besides these, prevention of occupational exposure by
managing blood and different body substances and providing a complete a risk assessment
guidelines to the hospital staff related to exposure prone procedures is also used (Slimings et al.,
2014). Further, there are also suggestions of using policies and protocols to regularly monitor the
effectiveness of infection prevention policies, which will be reviewed by the highest authority of
provides an opportunity to the pathogen to adapt and spread within a number of individuals.
Hence, each year Healthcare associated infections are recorded in a large number of patients
making it as the most common concern of hospitals (Cimiotti et al., 2012). However, it has been
seen that majority of the Healthcare associated infections are preventable and researchers believe
that there are mechanism through which these Hospital acquired infections can be minimised.
Successful infection control strategy requires cumulative effort of all the approaches such as
infection control hygienic surveillance safe and appropriate use of antibiotics and antimicrobial
stewardship (Magill et al., 2014).
While discussing the risk of clinical care activity related to standard 3 the impact of low
quality care and process to improve it should be discussed. Several strategies have been
mentioned to prevent and control the Healthcare associated infection, which are being developed
and implemented by Healthcare facilities in Australia. The first risk associated with effective
governance and management system for Healthcare associated infection. Laxminarayan et al.,
(2013) determine that developing and implementation of effective governance system for
infection prevention and control can help to decrease the risk of Healthcare associated infections
in patients. To achieve this, several approaches that can be taken and implemented as policy or
procedures such as using different aseptic techniques, using the standard related to infection
control, proper processing of reusable medical devices, cleaning and maintaining an adequate
environment through disinfection. Besides these, prevention of occupational exposure by
managing blood and different body substances and providing a complete a risk assessment
guidelines to the hospital staff related to exposure prone procedures is also used (Slimings et al.,
2014). Further, there are also suggestions of using policies and protocols to regularly monitor the
effectiveness of infection prevention policies, which will be reviewed by the highest authority of
6PROFESSIONAL NURSING PRACTICE
the organisation. The second risk associated with standard 3 is the infection within the
Healthcare facility and strategies for it. According to Yip et al., (2012) it can be achieved by
developing and implementing strict hand hygiene program or risk oriented work force
immunization programme with compliance with the National Health and Medical Research
Council guidelines of Australia. Compliance with the system will help to record the
communicable disease status and the workforce will be immunised so that patients did not
acquire Healthcare associated infections from the workforce (Drewe et al., 2012). The
Healthcare facility can also strictly implement strategies such as usage of personal protective
equipments, occupational health and safety policy so that disease cannot be spread through the
medical processes.
The third risk associated with preventing and controlling healthcare-associated infection
can be inability of the Healthcare facilities to track and control the Healthcare associated
infections within their environment. To overcome this risk, development and implementation of
regular review process should be used such as the antimicrobial stewardship system. Using this
the Healthcare facility will be able to track the prescribed antimicrobial medicines as per their
therapeutic guidelines and the resistance related risk. The fourth risk can be the environment of
the Healthcare facility using which, infection can be spread to patients and hence action should
be taken in a clean and hygienic environment in the Healthcare facility (Bereket et al., 2012).
This can be achieved by implementation of risk management system through which the
Healthcare facility can be maintained, the resources and the services will be managed. Further all
the risk of infection communication such as laundry linen, transportation, personal protective
equipments, infectious biological agents such as blood or bodily fluids will be cleaned using
disinfectants. As well as the reusable medical equipments will be cleaned, disinfectant and
the organisation. The second risk associated with standard 3 is the infection within the
Healthcare facility and strategies for it. According to Yip et al., (2012) it can be achieved by
developing and implementing strict hand hygiene program or risk oriented work force
immunization programme with compliance with the National Health and Medical Research
Council guidelines of Australia. Compliance with the system will help to record the
communicable disease status and the workforce will be immunised so that patients did not
acquire Healthcare associated infections from the workforce (Drewe et al., 2012). The
Healthcare facility can also strictly implement strategies such as usage of personal protective
equipments, occupational health and safety policy so that disease cannot be spread through the
medical processes.
The third risk associated with preventing and controlling healthcare-associated infection
can be inability of the Healthcare facilities to track and control the Healthcare associated
infections within their environment. To overcome this risk, development and implementation of
regular review process should be used such as the antimicrobial stewardship system. Using this
the Healthcare facility will be able to track the prescribed antimicrobial medicines as per their
therapeutic guidelines and the resistance related risk. The fourth risk can be the environment of
the Healthcare facility using which, infection can be spread to patients and hence action should
be taken in a clean and hygienic environment in the Healthcare facility (Bereket et al., 2012).
This can be achieved by implementation of risk management system through which the
Healthcare facility can be maintained, the resources and the services will be managed. Further all
the risk of infection communication such as laundry linen, transportation, personal protective
equipments, infectious biological agents such as blood or bodily fluids will be cleaned using
disinfectants. As well as the reusable medical equipments will be cleaned, disinfectant and
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7PROFESSIONAL NURSING PRACTICE
sterilized, so that the risk related to those can be minimised (Graber, 2013). The fifth clinical
care activity related to Healthcare associated infection will be health in literacy of patients that
will affect the health care service by increasing the risk of disease spread. This risk can be
minimised by providing the patients with consumer specific Healthcare information that will
help to minimise patients-related infection risk (Naujokas et al., 2013).
Several literatures have been focused on the processes and outcomes of the strategies
used to collect the data related to Healthcare associated infection within which surveillance is the
most appropriate method. The National Health and Medical Research Council have published a
report in which the role of surveillance introducing the Healthcare associated infection has been
mentioned (Kohl 3rd et al., 2012). According to that, surveillance is an important and wide array
system within the quality management of Healthcare facility having the primary aim of
collecting data so that health quality can be improved within the Healthcare facility. According
to Bloland et al. (2012), collection of such data helps to provide strategy to change or improve
the process and evaluate the effectiveness of it. For example, if and Healthcare facility wants to
improve its hand hygiene related practices, it should monitor its existing hand hygiene process
and comply it with the rate of infections related to blood stream, hand hygiene and so on.
Therefore, using surveillance the Healthcare facilities can collect different information about the
Healthcare environment and risk factors that promotes Healthcare associated infections
frequently (Naujokas et al., 2013). Secondly, it enables the facility to identify different steps that
can be used for prevention and control purpose and carry out timely investigation or audit for
sustainable prevention and control measures. Surveillance cycle such as data collection data
analysis, interpretation and dissemination helps to collect data related to Healthcare associated
infection and implement different strategies so that those infections can be prevented. There are
sterilized, so that the risk related to those can be minimised (Graber, 2013). The fifth clinical
care activity related to Healthcare associated infection will be health in literacy of patients that
will affect the health care service by increasing the risk of disease spread. This risk can be
minimised by providing the patients with consumer specific Healthcare information that will
help to minimise patients-related infection risk (Naujokas et al., 2013).
Several literatures have been focused on the processes and outcomes of the strategies
used to collect the data related to Healthcare associated infection within which surveillance is the
most appropriate method. The National Health and Medical Research Council have published a
report in which the role of surveillance introducing the Healthcare associated infection has been
mentioned (Kohl 3rd et al., 2012). According to that, surveillance is an important and wide array
system within the quality management of Healthcare facility having the primary aim of
collecting data so that health quality can be improved within the Healthcare facility. According
to Bloland et al. (2012), collection of such data helps to provide strategy to change or improve
the process and evaluate the effectiveness of it. For example, if and Healthcare facility wants to
improve its hand hygiene related practices, it should monitor its existing hand hygiene process
and comply it with the rate of infections related to blood stream, hand hygiene and so on.
Therefore, using surveillance the Healthcare facilities can collect different information about the
Healthcare environment and risk factors that promotes Healthcare associated infections
frequently (Naujokas et al., 2013). Secondly, it enables the facility to identify different steps that
can be used for prevention and control purpose and carry out timely investigation or audit for
sustainable prevention and control measures. Surveillance cycle such as data collection data
analysis, interpretation and dissemination helps to collect data related to Healthcare associated
infection and implement different strategies so that those infections can be prevented. There are
8PROFESSIONAL NURSING PRACTICE
several types of surveillance program that focus on specific populations, specific site of
infection, specific type of organism or specific location in the hospital or community where
Healthcare associated infection occurs (Drewe et al., 2012). Further using two methods for
surveillance such as process and outcome, the calculations of valid infection rates were done.
The process of surveillance includes precise identification of service event, systematic collection
of data, analysis and interpretation about the risk. Several steps should be used for Healthcare
associated infection surveillance (Graber, 2013). Firstly, the infection should be understood
properly so that from a pool of Healthcare associated infections, a particular infection can be
chosen for data collection and Management. The laboratory based data and Healthcare
prescriptions can be used for standardization. Thirdly, epidemiological important variables
should be collected such as population specific risk factors, serious adverse outcomes after
collection of the data analysis should be done (Kohl et al., 2012). So that increased rates of
transmission can be indicated for the feedback, information on the trend of the risk should be
provided and probable risk factor and related prevention strategies should be implemented.
The Australian Commission on Safety and Quality in Health Care (ACSQHC) directs and
manages national developments in safety and quality in health care. For the purpose, the
development of a service framework for safe and high quality care was developed using three
primary aspects such as consumer-centered care, information driven process, and organized for
safety. This framework was the National Healthcare Safety and Quality Service standards that
were divided in ten standards related to the healthcare processes. The primary aim of these
standards was to protect patients from healthcare harms, manage, and improve quality healthcare
services. In this assignment, the standard three of the healthcare standard was chosen for
discussion and clinical care activities that can lead to healthcare associated infections was
several types of surveillance program that focus on specific populations, specific site of
infection, specific type of organism or specific location in the hospital or community where
Healthcare associated infection occurs (Drewe et al., 2012). Further using two methods for
surveillance such as process and outcome, the calculations of valid infection rates were done.
The process of surveillance includes precise identification of service event, systematic collection
of data, analysis and interpretation about the risk. Several steps should be used for Healthcare
associated infection surveillance (Graber, 2013). Firstly, the infection should be understood
properly so that from a pool of Healthcare associated infections, a particular infection can be
chosen for data collection and Management. The laboratory based data and Healthcare
prescriptions can be used for standardization. Thirdly, epidemiological important variables
should be collected such as population specific risk factors, serious adverse outcomes after
collection of the data analysis should be done (Kohl et al., 2012). So that increased rates of
transmission can be indicated for the feedback, information on the trend of the risk should be
provided and probable risk factor and related prevention strategies should be implemented.
The Australian Commission on Safety and Quality in Health Care (ACSQHC) directs and
manages national developments in safety and quality in health care. For the purpose, the
development of a service framework for safe and high quality care was developed using three
primary aspects such as consumer-centered care, information driven process, and organized for
safety. This framework was the National Healthcare Safety and Quality Service standards that
were divided in ten standards related to the healthcare processes. The primary aim of these
standards was to protect patients from healthcare harms, manage, and improve quality healthcare
services. In this assignment, the standard three of the healthcare standard was chosen for
discussion and clinical care activities that can lead to healthcare associated infections was
9PROFESSIONAL NURSING PRACTICE
determined. Further, the approaches to manage those risks, as per the standard three of NHSQS
were determined. Besides these, the critical discussion of quality and safety issues related to
Australian healthcare system was determined. Finally a detailed discussion on the process and
outcome measurements such as surveillance was proposed for data collection and measurement
and its effectiveness was determined.
determined. Further, the approaches to manage those risks, as per the standard three of NHSQS
were determined. Besides these, the critical discussion of quality and safety issues related to
Australian healthcare system was determined. Finally a detailed discussion on the process and
outcome measurements such as surveillance was proposed for data collection and measurement
and its effectiveness was determined.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
10PROFESSIONAL NURSING PRACTICE
References
Australian Commission on Safety and Quality in Healthcare. (2018). The State of Safety and
Quality in Australian Health Care. Retrieved from
https://www.safetyandquality.gov.au/wp-content/uploads/2016/11/Vital-Signs-2016-
PDF.pdf
Australian Private Hospitals Association. (2018). Annual Reports - Australian Private Hospitals
Association. Retrieved from http://www.apha.org.au/about-apha/annual-reports/
Bereket, W., Hemalatha, K., Getenet, B., Wondwossen, T., Solomon, A., Zeynudin, A., &
Kannan, S. (2012). Update on bacterial nosocomial infections. Eur Rev Med Pharmacol
Sci, Vol. 16, issue 8, pp. 1039-44.
https://pdfs.semanticscholar.org/a121/0d5cec55ba8adc1a30a5e9a90c4082d3673e.pdf
Bloland, P., Simone, P., Burkholder, B., Slutsker, L., & De Cock, K. M. (2012). The role of
public health institutions in global health system strengthening efforts: the US CDC's
perspective. PLoS medicine,Vol 9, issue 4, pp. e1001199. DOI:
https://doi.org/10.1371/journal.pmed.1001199
Cimiotti, J. P., Aiken, L. H., Sloane, D. M., & Wu, E. S. (2012). Nurse staffing, burnout, and
health care–associated infection. American journal of infection control, Vol 40, issue 6,
pp. 486-490. DOI: https://doi.org/10.1016/j.ajic.2012.02.029
Drewe, J. A., Hoinville, L. J., Cook, A. J. C., Floyd, T., & Stärk, K. D. C. (2012). Evaluation of
animal and public health surveillance systems: a systematic review. Epidemiology &
Infection, Vol. 140, issue 4, pp. 575-590. DOI:
https://doi.org/10.1017/S0950268811002160
References
Australian Commission on Safety and Quality in Healthcare. (2018). The State of Safety and
Quality in Australian Health Care. Retrieved from
https://www.safetyandquality.gov.au/wp-content/uploads/2016/11/Vital-Signs-2016-
PDF.pdf
Australian Private Hospitals Association. (2018). Annual Reports - Australian Private Hospitals
Association. Retrieved from http://www.apha.org.au/about-apha/annual-reports/
Bereket, W., Hemalatha, K., Getenet, B., Wondwossen, T., Solomon, A., Zeynudin, A., &
Kannan, S. (2012). Update on bacterial nosocomial infections. Eur Rev Med Pharmacol
Sci, Vol. 16, issue 8, pp. 1039-44.
https://pdfs.semanticscholar.org/a121/0d5cec55ba8adc1a30a5e9a90c4082d3673e.pdf
Bloland, P., Simone, P., Burkholder, B., Slutsker, L., & De Cock, K. M. (2012). The role of
public health institutions in global health system strengthening efforts: the US CDC's
perspective. PLoS medicine,Vol 9, issue 4, pp. e1001199. DOI:
https://doi.org/10.1371/journal.pmed.1001199
Cimiotti, J. P., Aiken, L. H., Sloane, D. M., & Wu, E. S. (2012). Nurse staffing, burnout, and
health care–associated infection. American journal of infection control, Vol 40, issue 6,
pp. 486-490. DOI: https://doi.org/10.1016/j.ajic.2012.02.029
Drewe, J. A., Hoinville, L. J., Cook, A. J. C., Floyd, T., & Stärk, K. D. C. (2012). Evaluation of
animal and public health surveillance systems: a systematic review. Epidemiology &
Infection, Vol. 140, issue 4, pp. 575-590. DOI:
https://doi.org/10.1017/S0950268811002160
11PROFESSIONAL NURSING PRACTICE
Graber, M. L. (2013). The incidence of diagnostic error in medicine. BMJ Qual Saf, bmjqs-2012.
doi: 10.1136/bmjqs-2012-001615
Greenfield, D., Pawsey, M., Hinchcliff, R., Moldovan, M., & Braithwaite, J. (2012). The
standard of healthcare accreditation standards: a review of empirical research
underpinning their development and impact. BMC health services research, Vol. 12,
issue 1, pp. 329. DOI: https://doi.org/10.1186/1472-6963-12-329
Kohl 3rd, H. W., Craig, C. L., Lambert, E. V., Inoue, S., Alkandari, J. R., Leetongin, G., ... &
Lancet Physical Activity Series Working Group. (2012). The pandemic of physical
inactivity: global action for public health. The Lancet, Vol. 380, issue 9838, pp. 294-305.
https://doi.org/10.1016/S0140-6736(12)60898-8
Laxminarayan, R., Duse, A., Wattal, C., Zaidi, A. K., Wertheim, H. F., Sumpradit, N., ... &
Greko, C. (2013). Antibiotic resistance—the need for global solutions. The Lancet
infectious diseases, Vol. 13, issue 12, pp. 1057-1098. DOI:
https://doi.org/10.1016/S1473-3099(13)70318-9
Magill, S. S., Edwards, J. R., Bamberg, W., Beldavs, Z. G., Dumyati, G., Kainer, M. A., ... &
Ray, S. M. (2014). Multistate point-prevalence survey of health care–associated
infections. New England Journal of Medicine, Vol. 370, issue 13, pp. 1198-1208. DOI:
10.1056/NEJMoa1306801
McSHERRY, R. O. B. E. R. T., Pearce, P., Grimwood, K., & McSherry, W. (2012). The pivotal
role of nurse managers, leaders and educators in enabling excellence in nursing
care. Journal of Nursing Management, vol 20, issue 1, pp. 7-19. DOI:
https://doi.org/10.1111/j.1365-2834.2011.01349.x
Graber, M. L. (2013). The incidence of diagnostic error in medicine. BMJ Qual Saf, bmjqs-2012.
doi: 10.1136/bmjqs-2012-001615
Greenfield, D., Pawsey, M., Hinchcliff, R., Moldovan, M., & Braithwaite, J. (2012). The
standard of healthcare accreditation standards: a review of empirical research
underpinning their development and impact. BMC health services research, Vol. 12,
issue 1, pp. 329. DOI: https://doi.org/10.1186/1472-6963-12-329
Kohl 3rd, H. W., Craig, C. L., Lambert, E. V., Inoue, S., Alkandari, J. R., Leetongin, G., ... &
Lancet Physical Activity Series Working Group. (2012). The pandemic of physical
inactivity: global action for public health. The Lancet, Vol. 380, issue 9838, pp. 294-305.
https://doi.org/10.1016/S0140-6736(12)60898-8
Laxminarayan, R., Duse, A., Wattal, C., Zaidi, A. K., Wertheim, H. F., Sumpradit, N., ... &
Greko, C. (2013). Antibiotic resistance—the need for global solutions. The Lancet
infectious diseases, Vol. 13, issue 12, pp. 1057-1098. DOI:
https://doi.org/10.1016/S1473-3099(13)70318-9
Magill, S. S., Edwards, J. R., Bamberg, W., Beldavs, Z. G., Dumyati, G., Kainer, M. A., ... &
Ray, S. M. (2014). Multistate point-prevalence survey of health care–associated
infections. New England Journal of Medicine, Vol. 370, issue 13, pp. 1198-1208. DOI:
10.1056/NEJMoa1306801
McSHERRY, R. O. B. E. R. T., Pearce, P., Grimwood, K., & McSherry, W. (2012). The pivotal
role of nurse managers, leaders and educators in enabling excellence in nursing
care. Journal of Nursing Management, vol 20, issue 1, pp. 7-19. DOI:
https://doi.org/10.1111/j.1365-2834.2011.01349.x
12PROFESSIONAL NURSING PRACTICE
National Safety and Quality Health Service Standards. (2012). National Safety and Quality
Health Service Standards. Retrieved from https://www.safetyandquality.gov.au/wp-
content/uploads/2011/09/NSQHS-Standards-Sept-2012.pdf
Naujokas, M. F., Anderson, B., Ahsan, H., Aposhian, H. V., Graziano, J. H., Thompson, C., &
Suk, W. A. (2013). The broad scope of health effects from chronic arsenic exposure:
update on a worldwide public health problem. Environmental health perspectives, Vol.
121, issue 3, pp. 295. Doi: 10.1289/ehp.1205875
Runciman, W. B., Hunt, T. D., Hannaford, N. A., Hibbert, P. D., Westbrook, J. I., Coiera, E.
W., ... & Braithwaite, J. (2012). CareTrack: assessing the appropriateness of health care
delivery in Australia. Medical Journal of Australia, Vol. 197, issue 2, pp. 100. Retrieved
from: https://www.mja.com.au/system/files/issues/197_02_160712/run10510_fm.pdf
Slimings, C., Armstrong, P., Beckingham, W. D., Bull, A. L., Hall, L., Kennedy, K. J., ... &
Richards, M. J. (2014). Increasing incidence of Clostridium difficile infection, Australia,
2011–2012. The Medical Journal of Australia, Vol. 200, issue 5, pp. 272-276. Retrieved
from: https://www.mja.com.au/system/files/issues/200_05_170314/sli11153_fm.pdf
Yip, W. C. M., Hsiao, W. C., Chen, W., Hu, S., Ma, J., & Maynard, A. (2012). Early appraisal of
China's huge and complex health-care reforms. The Lancet, Vol. 379, issue 9818, pp.
833-842. DOI: https://doi.org/10.1016/S0140-6736(11)61880-1
Zingg, W., Holmes, A., Dettenkofer, M., Goetting, T., Secci, F., Clack, L., ... & Pittet, D. (2015).
Hospital organisation, management, and structure for prevention of health-care-
associated infection: a systematic review and expert consensus. The Lancet Infectious
Diseases, VFol. 15, issue 2, pp. 212-224. DOI: https://doi.org/10.1016/S1473-
3099(14)70854-0
National Safety and Quality Health Service Standards. (2012). National Safety and Quality
Health Service Standards. Retrieved from https://www.safetyandquality.gov.au/wp-
content/uploads/2011/09/NSQHS-Standards-Sept-2012.pdf
Naujokas, M. F., Anderson, B., Ahsan, H., Aposhian, H. V., Graziano, J. H., Thompson, C., &
Suk, W. A. (2013). The broad scope of health effects from chronic arsenic exposure:
update on a worldwide public health problem. Environmental health perspectives, Vol.
121, issue 3, pp. 295. Doi: 10.1289/ehp.1205875
Runciman, W. B., Hunt, T. D., Hannaford, N. A., Hibbert, P. D., Westbrook, J. I., Coiera, E.
W., ... & Braithwaite, J. (2012). CareTrack: assessing the appropriateness of health care
delivery in Australia. Medical Journal of Australia, Vol. 197, issue 2, pp. 100. Retrieved
from: https://www.mja.com.au/system/files/issues/197_02_160712/run10510_fm.pdf
Slimings, C., Armstrong, P., Beckingham, W. D., Bull, A. L., Hall, L., Kennedy, K. J., ... &
Richards, M. J. (2014). Increasing incidence of Clostridium difficile infection, Australia,
2011–2012. The Medical Journal of Australia, Vol. 200, issue 5, pp. 272-276. Retrieved
from: https://www.mja.com.au/system/files/issues/200_05_170314/sli11153_fm.pdf
Yip, W. C. M., Hsiao, W. C., Chen, W., Hu, S., Ma, J., & Maynard, A. (2012). Early appraisal of
China's huge and complex health-care reforms. The Lancet, Vol. 379, issue 9818, pp.
833-842. DOI: https://doi.org/10.1016/S0140-6736(11)61880-1
Zingg, W., Holmes, A., Dettenkofer, M., Goetting, T., Secci, F., Clack, L., ... & Pittet, D. (2015).
Hospital organisation, management, and structure for prevention of health-care-
associated infection: a systematic review and expert consensus. The Lancet Infectious
Diseases, VFol. 15, issue 2, pp. 212-224. DOI: https://doi.org/10.1016/S1473-
3099(14)70854-0
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

13PROFESSIONAL NURSING PRACTICE
1 out of 14
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.