Safe Urine Sample Collection and Analysis
VerifiedAdded on 2021/04/16
|9
|1565
|43
AI Summary
This assignment involves the analysis of a patient's urine test results, which indicate the presence of nitrites and moderate protein levels. The student must identify potential health issues, such as urinary tract infections or kidney disease, and discuss the importance of safe sample collection and quick analytical skills in diagnosing patients accurately.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.

Running head: URINALYSIS
Urinalysis
Name of Student
Name of University
Author Note
Urinalysis
Name of Student
Name of University
Author Note
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
1Urinalysis
Urinalysis is a diagnostic procedure of analysis urine through clinical trials in many
healthcare settings, clinical laboratories advised by clinical practitioners to identify presence of
imbalance in the body of an individual (Delanghe and Speeckaert 2014). The excretory system of
the body is extremely important to determine homeostatic conditions of the body by eliminating
waste keeping the balance between fluids and impure substances out of the body and maintaining
the ionic interactions. Change in homeostasis will have direct effect on the urine as, color
change, smell and presence of biochemical substances and their amounts to determine any
diseased condition (McCarron et al. 2013). This test is very useful to determine Urinary tract
infection (UTI), kidney diseases, determining pregnancy and mapping hormonal changes.
There are three ways to collect clinical sample, Midstream Specimen Collection for
adults, Catheter collection from elderly and disabled patients and Pediatric collection from
babies and infants (Altuntas et al. 2015). Proper instructions should be given to all patients and
made sure no patient is at unrest or discomfort before the test and hands should be washed and
sterilized throughout the procedure and the collected sample should be properly stored.
The Dipstick analysis is performed using various parameters like, presence of leucocytes,
blood, nitrites, glucose, protein, bilirubin, ketones and urobilinogen content (Stein et al. 2015).
Sometimes the pH and specific gravity may also be diagnosed. The clinical stick contains small
patches of various chemicals that can determine the presence of the above-mentioned substances.
Leucocytes are thought to be present in urine due to formation of pus, from dead white
blood cells, hinting at an undetected renal problem. This condition is called pyuria, which needs
to be properly examined under microscope or the urine sample can be inoculated to prepare a
bacterial culture to ensure the commencement of antibiotic treatment (Hilt et al. 2014).
Urinalysis is a diagnostic procedure of analysis urine through clinical trials in many
healthcare settings, clinical laboratories advised by clinical practitioners to identify presence of
imbalance in the body of an individual (Delanghe and Speeckaert 2014). The excretory system of
the body is extremely important to determine homeostatic conditions of the body by eliminating
waste keeping the balance between fluids and impure substances out of the body and maintaining
the ionic interactions. Change in homeostasis will have direct effect on the urine as, color
change, smell and presence of biochemical substances and their amounts to determine any
diseased condition (McCarron et al. 2013). This test is very useful to determine Urinary tract
infection (UTI), kidney diseases, determining pregnancy and mapping hormonal changes.
There are three ways to collect clinical sample, Midstream Specimen Collection for
adults, Catheter collection from elderly and disabled patients and Pediatric collection from
babies and infants (Altuntas et al. 2015). Proper instructions should be given to all patients and
made sure no patient is at unrest or discomfort before the test and hands should be washed and
sterilized throughout the procedure and the collected sample should be properly stored.
The Dipstick analysis is performed using various parameters like, presence of leucocytes,
blood, nitrites, glucose, protein, bilirubin, ketones and urobilinogen content (Stein et al. 2015).
Sometimes the pH and specific gravity may also be diagnosed. The clinical stick contains small
patches of various chemicals that can determine the presence of the above-mentioned substances.
Leucocytes are thought to be present in urine due to formation of pus, from dead white
blood cells, hinting at an undetected renal problem. This condition is called pyuria, which needs
to be properly examined under microscope or the urine sample can be inoculated to prepare a
bacterial culture to ensure the commencement of antibiotic treatment (Hilt et al. 2014).
2Urinalysis
Presence of blood in urine is an indication of an abnormal condition unless the patient is a
female undergoing her menstruation cycle. Presence of blood in urine is an alarming condition
which is described as hematuria, caused when the renal system is undergoing any inflammatory
disease or trauma, like kidney stones or cancer formation (Foxman 2013). Hemolytic conditions
can also result in presence of blood in urine, known as Hemoglobinuria.
Presence of nitrites in urine usually signifies presence of microorganisms in the renal
system that can convert nitrate substances into nitrites (Stein 2015).
Elevated levels of glucose or sugar are usually related to diabetes. The allowed level of
glucose in renal cavity is 10-11mmols. Presence of glucose higher than the threshold amount in
urine is called Glycosuria (Bispo et al. 2013). Patients who are administered with corticosteroids
can also show elevated levels of glucose in their urine.
Proteins are generally too large to pass through the filtration barrier of glomerulus in
kidney. The process of escape of protein through the glomerulus into the excreted urine is called
Proteinuria (Free 2018). Many conditions can lead to expansion of the glomerulus filters like,
diabetes mellitus, possible functional damage of kidney, hyperthyroidism, hypertension and
jaundice.
Ketones are formed after breakdown of fats, particularly in cases of prolonged starvation,
low carbohydrate diets, high protein. Patients with a diabetic condition also may have ketones in
their urine due to lack of insulin, which transports glucose inside the cells. Ketonuria occurs
when excessive fat is burned in the body. (Free 2018). Usually patients with such conditions
show other symptoms like vomiting and diarrhea. Certain pharmaceutical medicines like
captropil also interfere with the presence of glucose in urine.
Presence of blood in urine is an indication of an abnormal condition unless the patient is a
female undergoing her menstruation cycle. Presence of blood in urine is an alarming condition
which is described as hematuria, caused when the renal system is undergoing any inflammatory
disease or trauma, like kidney stones or cancer formation (Foxman 2013). Hemolytic conditions
can also result in presence of blood in urine, known as Hemoglobinuria.
Presence of nitrites in urine usually signifies presence of microorganisms in the renal
system that can convert nitrate substances into nitrites (Stein 2015).
Elevated levels of glucose or sugar are usually related to diabetes. The allowed level of
glucose in renal cavity is 10-11mmols. Presence of glucose higher than the threshold amount in
urine is called Glycosuria (Bispo et al. 2013). Patients who are administered with corticosteroids
can also show elevated levels of glucose in their urine.
Proteins are generally too large to pass through the filtration barrier of glomerulus in
kidney. The process of escape of protein through the glomerulus into the excreted urine is called
Proteinuria (Free 2018). Many conditions can lead to expansion of the glomerulus filters like,
diabetes mellitus, possible functional damage of kidney, hyperthyroidism, hypertension and
jaundice.
Ketones are formed after breakdown of fats, particularly in cases of prolonged starvation,
low carbohydrate diets, high protein. Patients with a diabetic condition also may have ketones in
their urine due to lack of insulin, which transports glucose inside the cells. Ketonuria occurs
when excessive fat is burned in the body. (Free 2018). Usually patients with such conditions
show other symptoms like vomiting and diarrhea. Certain pharmaceutical medicines like
captropil also interfere with the presence of glucose in urine.
3Urinalysis
Presence of bile pigments like Bilirubin and urobilinogen changes the color or urine and
makes it darker. Bilirubin is formed when erythrocytes are broken down, but they cannot pass
through the glomerulus filtration system so they are transported to liver, where it is further
broken down into water-soluble glucoronic acid which is easily excreted. The presence of this
bile pigment is suggestive of liver failure or due o obstruction in the bile duct (Singh 2013).
Excessive amounts of urobilinogen in urine signify that the patient is undergoing internal
pathogenic infection.
The pH of urine is normally acidic in nature with optimal range form 5.0-8.0. Any
lowering or increase in this range is considered problematic (Delanghe and Speeckaert 2014).
Increase in acidity of the urine signifies presence of kidney stones or dietary imbalance, protein
or dairy rich diet makes urine acidic. Increasing the pH, that is increase in alkalinity of the urine
indicates that the patient may be suffering from pathogenic infection like, Klebshiella, Proteus or
Pseudomonas infection.
Urinalysis also involves comparing the specific gravity of the liquid to ensure the ratio
between solute and solvent is within threshold levels (Delanghe and Speeckaert 2014). The
allowed range is 1.001-1.035. Increase in the specific gravity of urine of a patient signifies the
patient is in dehydrated condition. Patients with diabetes incipidus are recorded to lower and
diluted levels of urine. Hypercalcaemic patients also have diluted levels of urine.
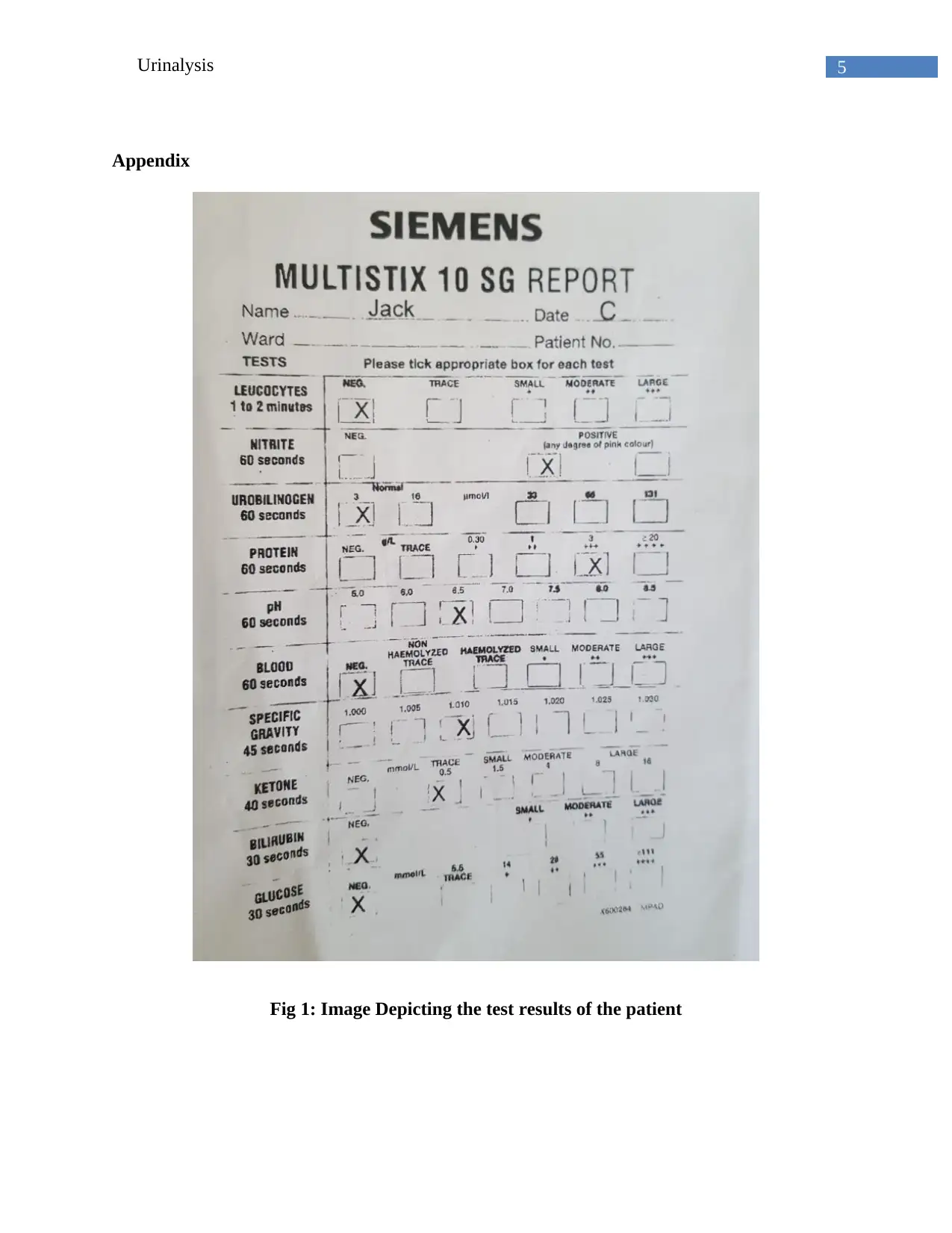
The patient in question Appendix: Fig 1, of the case provided have presence of nitrites
and moderate presence of proteins. This suggests that the patient might be suffering from a
possible urinary tract infection and the sample should be sent to a microbiology lab immediately.
Absence of any detectable microorganism in urine would imply that the patient is suffering from
Presence of bile pigments like Bilirubin and urobilinogen changes the color or urine and
makes it darker. Bilirubin is formed when erythrocytes are broken down, but they cannot pass
through the glomerulus filtration system so they are transported to liver, where it is further
broken down into water-soluble glucoronic acid which is easily excreted. The presence of this
bile pigment is suggestive of liver failure or due o obstruction in the bile duct (Singh 2013).
Excessive amounts of urobilinogen in urine signify that the patient is undergoing internal
pathogenic infection.
The pH of urine is normally acidic in nature with optimal range form 5.0-8.0. Any
lowering or increase in this range is considered problematic (Delanghe and Speeckaert 2014).
Increase in acidity of the urine signifies presence of kidney stones or dietary imbalance, protein
or dairy rich diet makes urine acidic. Increasing the pH, that is increase in alkalinity of the urine
indicates that the patient may be suffering from pathogenic infection like, Klebshiella, Proteus or
Pseudomonas infection.
Urinalysis also involves comparing the specific gravity of the liquid to ensure the ratio
between solute and solvent is within threshold levels (Delanghe and Speeckaert 2014). The
allowed range is 1.001-1.035. Increase in the specific gravity of urine of a patient signifies the
patient is in dehydrated condition. Patients with diabetes incipidus are recorded to lower and
diluted levels of urine. Hypercalcaemic patients also have diluted levels of urine.
The patient in question Appendix: Fig 1, of the case provided have presence of nitrites
and moderate presence of proteins. This suggests that the patient might be suffering from a
possible urinary tract infection and the sample should be sent to a microbiology lab immediately.
Absence of any detectable microorganism in urine would imply that the patient is suffering from
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
4Urinalysis
kidney disease, that needs to be addressed immediately, and special dietary restrictions are to be
placed on the patient. All other parameters seem to be within threshold range.
From the above observation, Appendix: Fig: 1, considering all possible outcomes I can
suggest that the governing nurse should be careful to perform the urine sample collection. I think
that, as a nurse it is my duty to perform the clinical test with much safety as possible in order to
avoid any contamination. If any diagnostic help is required from a senior health practitioner, I
should inform them immediately. Safe handling, quick analytical skills will ensure safe diagnosis
of an ailing patient is a duty of a nurse.
kidney disease, that needs to be addressed immediately, and special dietary restrictions are to be
placed on the patient. All other parameters seem to be within threshold range.
From the above observation, Appendix: Fig: 1, considering all possible outcomes I can
suggest that the governing nurse should be careful to perform the urine sample collection. I think
that, as a nurse it is my duty to perform the clinical test with much safety as possible in order to
avoid any contamination. If any diagnostic help is required from a senior health practitioner, I
should inform them immediately. Safe handling, quick analytical skills will ensure safe diagnosis
of an ailing patient is a duty of a nurse.
5Urinalysis
Appendix
Fig 1: Image Depicting the test results of the patient
Appendix
Fig 1: Image Depicting the test results of the patient

6Urinalysis
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7Urinalysis
References:
Altuntas, N., Tayfur, A.C., Kocak, M., Razi, H.C. and Akkurt, S., 2015. Midstream clean-catch
urine collection in newborns: a randomized controlled study. European journal of
pediatrics, 174(5), pp.577-582.
Bispo, J.A.M., de Sousa Vieira, E.E., Silveira, L. and Fernandes, A.B., 2013. Correlating the
amount of urea, creatinine, and glucose in urine from patients with diabetes mellitus and
hypertension with the risk of developing renal lesions by means of Raman spectroscopy and
principal component analysis. Journal of biomedical optics, 18(8), p.087004.
Delanghe, J. and Speeckaert, M., 2014. Preanalytical requirements of urinalysis. Biochemia
medica: Biochemia medica, 24(1), pp.89-104.
Foxman, B., 2013. Urinary tract infection. In Women and Health (Second Edition) (pp. 553-564).
Free, H.M., 2018. Urinalysis in clinical laboratory practice. Crc Press.
Hilt, E.E., McKinley, K., Pearce, M.M., Rosenfeld, A.B., Zilliox, M.J., Mueller, E.R., Brubaker,
L., Gai, X., Wolfe, A.J. and Schreckenberger, P.C., 2014. Urine is not sterile: use of enhanced
urine culture techniques to detect resident bacterial flora in the adult female bladder. Journal of
clinical microbiology, 52(3), pp.871-876.
McCarron, D.A., Kazaks, A.G., Geerling, J.C., Stern, J.S. and Graudal, N.A., 2013. Normal
range of human dietary sodium intake: a perspective based on 24-hour urinary sodium excretion
worldwide. American journal of hypertension, 26(10), pp.1218-1223.
References:
Altuntas, N., Tayfur, A.C., Kocak, M., Razi, H.C. and Akkurt, S., 2015. Midstream clean-catch
urine collection in newborns: a randomized controlled study. European journal of
pediatrics, 174(5), pp.577-582.
Bispo, J.A.M., de Sousa Vieira, E.E., Silveira, L. and Fernandes, A.B., 2013. Correlating the
amount of urea, creatinine, and glucose in urine from patients with diabetes mellitus and
hypertension with the risk of developing renal lesions by means of Raman spectroscopy and
principal component analysis. Journal of biomedical optics, 18(8), p.087004.
Delanghe, J. and Speeckaert, M., 2014. Preanalytical requirements of urinalysis. Biochemia
medica: Biochemia medica, 24(1), pp.89-104.
Foxman, B., 2013. Urinary tract infection. In Women and Health (Second Edition) (pp. 553-564).
Free, H.M., 2018. Urinalysis in clinical laboratory practice. Crc Press.
Hilt, E.E., McKinley, K., Pearce, M.M., Rosenfeld, A.B., Zilliox, M.J., Mueller, E.R., Brubaker,
L., Gai, X., Wolfe, A.J. and Schreckenberger, P.C., 2014. Urine is not sterile: use of enhanced
urine culture techniques to detect resident bacterial flora in the adult female bladder. Journal of
clinical microbiology, 52(3), pp.871-876.
McCarron, D.A., Kazaks, A.G., Geerling, J.C., Stern, J.S. and Graudal, N.A., 2013. Normal
range of human dietary sodium intake: a perspective based on 24-hour urinary sodium excretion
worldwide. American journal of hypertension, 26(10), pp.1218-1223.
8Urinalysis
Singh, K., 2013. Evaluation and interpretation of biomarkers of liver diseases. Int J Res Health
Sci, 1(3), pp.213-23.
Stein, R., Dogan, H.S., Hoebeke, P., Kočvara, R., Nijman, R.J., Radmayr, C. and Tekgül, S.,
2015. Urinary tract infections in children: EAU/ESPU guidelines. European urology, 67(3),
pp.546-558.
Waugh, A. and Grant, A., Anatomy and Physiology in Health and Illness–Text, Colouring Book
and Workbook Package.
Singh, K., 2013. Evaluation and interpretation of biomarkers of liver diseases. Int J Res Health
Sci, 1(3), pp.213-23.
Stein, R., Dogan, H.S., Hoebeke, P., Kočvara, R., Nijman, R.J., Radmayr, C. and Tekgül, S.,
2015. Urinary tract infections in children: EAU/ESPU guidelines. European urology, 67(3),
pp.546-558.
Waugh, A. and Grant, A., Anatomy and Physiology in Health and Illness–Text, Colouring Book
and Workbook Package.
1 out of 9
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.