SISSFFIT015 Portfolio Assessment: Case Study and Risk Factors
VerifiedAdded on 2023/06/12
|18
|5486
|393
AI Summary
This portfolio assessment for SISSFFIT015 includes a case study of a client who has been referred to a gym by a doctor after a motor vehicle accident. The assessment requires the student to provide a profile of a medical or allied health professional who could be chosen to communicate with about the case study client, prepare a letter to a relevant medical and/or allied health professional, and prepare a report to support this letter. Additionally, there is a true/false section on risk factors.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.
Assessment 1- Portfolio (SISSFFIT015)
Student Name: Marianna Sofianidou Student ID: CSF 160063
Assessment Type: Portfolio Other: Portfolio
Assessor’s Name:
Assessment
Outcome:
☐ Satisfactory ☐ Not Yet Satisfactory
Student
Declaration:
By submitting this assessment via Moodle, I declare that this is my own work and had
not been copied or plagiarised from any other source. Please refer to the Student
Handbook for more information.
Assessment
Conditions:
Each assessment criteria is recorded as either Satisfactory (S) or Not Yet Satisfactory
(NYS). A student can only achieve a ‘Satisfactory’ Assessment Outcome for the entire
assessment when all assessment Criteria listed below are ‘Satisfactory’. A student who
is assessed as ‘Not Yet Satisfactory’ is eligible for re-assessment with their trainer.
All assessment answers must be typed, include this assessment cover sheet and
uploaded in ‘WORD’ version to moodle.
Assessment Criteria
Element Performance Criteria S NYS
1. Refer to medical or
allied health
professional.
1.1 Analyse client pre-exercise screening, risk stratification, and
relevant fitness testing results.
☐ ☐
1.2 Collect relevant health information from client as required. ☐ ☐
1.3 Identify need for referral and guidance from medical practitioner
or appropriate allied health professional.
☐ ☐
1.4 Determine appropriate medical or allied health professional for
client referral.
☐ ☐
1.5 Obtain informed consent from client for the purpose of sharing
client information with health professionals, including referrals.
☐ ☐
1.6 Conduct referral in accordance with industry endorsed referral
procedures.
☐ ☐
2. Receive and
respond to referrals. 2.1 Receive guidance from medical or allied health professional. ☐ ☐
2.2 Seek verbal or written clarification from medical or allied health
professional, if required.
☐ ☐
2.3 Clarify recommendations with client and answer queries as
required.
☐ ☐
3. Deliver and monitor
client fitness program 3.1 Deliver exercise in accordance with guidance received from
medical or allied health professional, within industry endorsed scope
☐ ☐
VC001 College of Sports & Fitness - 11/05/2017- SISFFIT015
International College of Capoeira Pty Ltd trading as ’College of Sports & Fitness’ ABN 90 125 114 730/ Registered
Training Organisation 91345/ CRICOS Provider Code 03057C
Student Name: Marianna Sofianidou Student ID: CSF 160063
Assessment Type: Portfolio Other: Portfolio
Assessor’s Name:
Assessment
Outcome:
☐ Satisfactory ☐ Not Yet Satisfactory
Student
Declaration:
By submitting this assessment via Moodle, I declare that this is my own work and had
not been copied or plagiarised from any other source. Please refer to the Student
Handbook for more information.
Assessment
Conditions:
Each assessment criteria is recorded as either Satisfactory (S) or Not Yet Satisfactory
(NYS). A student can only achieve a ‘Satisfactory’ Assessment Outcome for the entire
assessment when all assessment Criteria listed below are ‘Satisfactory’. A student who
is assessed as ‘Not Yet Satisfactory’ is eligible for re-assessment with their trainer.
All assessment answers must be typed, include this assessment cover sheet and
uploaded in ‘WORD’ version to moodle.
Assessment Criteria
Element Performance Criteria S NYS
1. Refer to medical or
allied health
professional.
1.1 Analyse client pre-exercise screening, risk stratification, and
relevant fitness testing results.
☐ ☐
1.2 Collect relevant health information from client as required. ☐ ☐
1.3 Identify need for referral and guidance from medical practitioner
or appropriate allied health professional.
☐ ☐
1.4 Determine appropriate medical or allied health professional for
client referral.
☐ ☐
1.5 Obtain informed consent from client for the purpose of sharing
client information with health professionals, including referrals.
☐ ☐
1.6 Conduct referral in accordance with industry endorsed referral
procedures.
☐ ☐
2. Receive and
respond to referrals. 2.1 Receive guidance from medical or allied health professional. ☐ ☐
2.2 Seek verbal or written clarification from medical or allied health
professional, if required.
☐ ☐
2.3 Clarify recommendations with client and answer queries as
required.
☐ ☐
3. Deliver and monitor
client fitness program 3.1 Deliver exercise in accordance with guidance received from
medical or allied health professional, within industry endorsed scope
☐ ☐
VC001 College of Sports & Fitness - 11/05/2017- SISFFIT015
International College of Capoeira Pty Ltd trading as ’College of Sports & Fitness’ ABN 90 125 114 730/ Registered
Training Organisation 91345/ CRICOS Provider Code 03057C
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Assessment 1- Portfolio (SISSFFIT015)
of practice.
3.2 Monitor client responses to exercise and make appropriate
adjustments as required.
☐ ☐
3.3 Respond to signs and symptoms of exercise intolerance and take
appropriate action within scope of practice.
☐ ☐
3.4 Refer client to appropriate medical practitioner or allied health
professional if required.
☐ ☐
4. Report on client
progress. 4.1 Maintain records of client participation and progress. ☐ ☐
4.2 Provide feedback to relevant medical or allied health professional
in a timely manner using industry endorsed referral reporting
procedures.
☐ ☐
4.3 Receive further guidance from medical or allied health
professional and modify exercise program and delivery as required.
☐ ☐
4.4 Provide feedback to client on progress and any recommended
adjustments to exercise program.
☐ ☐
5. Maintain client
records. 5.1 Identify and record information for communication and reporting
to relevant medical or allied health professionals.
☐ ☐
5.2 Update and maintain current client. ☐ ☐
VC001 College of Sports & Fitness - 11/05/2017- SISFFIT015
International College of Capoeira Pty Ltd trading as ’College of Sports & Fitness’ ABN 90 125 114 730/ Registered
Training Organisation 91345/ CRICOS Provider Code 03057C
of practice.
3.2 Monitor client responses to exercise and make appropriate
adjustments as required.
☐ ☐
3.3 Respond to signs and symptoms of exercise intolerance and take
appropriate action within scope of practice.
☐ ☐
3.4 Refer client to appropriate medical practitioner or allied health
professional if required.
☐ ☐
4. Report on client
progress. 4.1 Maintain records of client participation and progress. ☐ ☐
4.2 Provide feedback to relevant medical or allied health professional
in a timely manner using industry endorsed referral reporting
procedures.
☐ ☐
4.3 Receive further guidance from medical or allied health
professional and modify exercise program and delivery as required.
☐ ☐
4.4 Provide feedback to client on progress and any recommended
adjustments to exercise program.
☐ ☐
5. Maintain client
records. 5.1 Identify and record information for communication and reporting
to relevant medical or allied health professionals.
☐ ☐
5.2 Update and maintain current client. ☐ ☐
VC001 College of Sports & Fitness - 11/05/2017- SISFFIT015
International College of Capoeira Pty Ltd trading as ’College of Sports & Fitness’ ABN 90 125 114 730/ Registered
Training Organisation 91345/ CRICOS Provider Code 03057C
Assessment 1- Portfolio (SISSFFIT015)
Part A
Case study – Provide referral (15 marks)
Task:
1. Provide a profile of a medical and/or allied health professional who could be chosen to
communicate with about the case study client outlined below. You will need to communicate
with a medical and/or allied health professional in regards to clearance before prescribing an
exercise program. This will depend on the type/s of medical and allied health professionals
chosen – that is, if the person is only suited to treating patients of a medical nature, an additional
letter and report to an allied health professional may be necessary. Outline their area of expertise
to justify your referral to this medical and/allied health professional. Provide evidence of your
communication with this medical and/or allied health professional.
2. Using the above information, prepare a letter to a relevant medical and/or allied health
professional in regards to the client’s results on his pre-exercise screening form. The letter is to
contain an introduction and an overview of your requirements – that is, you will require
clearance and guidance in order to deliver a fitness program for the client.
3. Prepare a report to support this letter that outlines:
● the results of the pre-exercise screening form and fitness test
● request for clearance to perform these exercises and activities, and/or clearance to perform
alternatives as suggested by the medical and/or allied health professional
● the client’s fitness goals and your view on his goals
● an outline of the client’s risk factors and why these risk factors are beyond your area of
expertise.
Case study – Peter
Peter is a 51-year-old male client at the gym. He has been referred from a doctor. He was recently
involved in a motor vehicle accident (three months ago). Peter suffered from a fractured tibia in the
car accident, which was operated on, and then placed in a plaster of Paris cast for six weeks. He has
recovered well from this operation. The bone is in good condition and cleared for exercise following
VC001 College of Sports & Fitness - 11/05/2017- SISFFIT015
International College of Capoeira Pty Ltd trading as ’College of Sports & Fitness’ ABN 90 125 114 730/ Registered
Training Organisation 91345/ CRICOS Provider Code 03057C
Part A
Case study – Provide referral (15 marks)
Task:
1. Provide a profile of a medical and/or allied health professional who could be chosen to
communicate with about the case study client outlined below. You will need to communicate
with a medical and/or allied health professional in regards to clearance before prescribing an
exercise program. This will depend on the type/s of medical and allied health professionals
chosen – that is, if the person is only suited to treating patients of a medical nature, an additional
letter and report to an allied health professional may be necessary. Outline their area of expertise
to justify your referral to this medical and/allied health professional. Provide evidence of your
communication with this medical and/or allied health professional.
2. Using the above information, prepare a letter to a relevant medical and/or allied health
professional in regards to the client’s results on his pre-exercise screening form. The letter is to
contain an introduction and an overview of your requirements – that is, you will require
clearance and guidance in order to deliver a fitness program for the client.
3. Prepare a report to support this letter that outlines:
● the results of the pre-exercise screening form and fitness test
● request for clearance to perform these exercises and activities, and/or clearance to perform
alternatives as suggested by the medical and/or allied health professional
● the client’s fitness goals and your view on his goals
● an outline of the client’s risk factors and why these risk factors are beyond your area of
expertise.
Case study – Peter
Peter is a 51-year-old male client at the gym. He has been referred from a doctor. He was recently
involved in a motor vehicle accident (three months ago). Peter suffered from a fractured tibia in the
car accident, which was operated on, and then placed in a plaster of Paris cast for six weeks. He has
recovered well from this operation. The bone is in good condition and cleared for exercise following
VC001 College of Sports & Fitness - 11/05/2017- SISFFIT015
International College of Capoeira Pty Ltd trading as ’College of Sports & Fitness’ ABN 90 125 114 730/ Registered
Training Organisation 91345/ CRICOS Provider Code 03057C
Assessment 1- Portfolio (SISSFFIT015)
some early rounds of physiotherapy. Peter’s doctor has recommended that he start going to the gym
to get fit and healthy again. Prior to his motor vehicle accident Peter walked daily, but he has never
exercised in a gym before. Peter reports feeling very tight in the calf muscles and ankle since the
plaster was removed six weeks ago. Peter’s other health information, as provided by his doctor,
includes:
● a blood pressure reading of 142/92 bpm
● asthma (he takes ventolin)
● poor eating habits, such as frequent takeaway lunches at work and dinner, skipping breakfast.
Note: Although this doctor has suggested that Peter join a gym, you should still assume that you will
require clearance from the relevant medical and/or allied health professionals prior to exercise
testing and/or programming when considering Peter’s medical and health status.
Referral letter from Health ProfessionaL TO Fitness Trainer
Practitioner Name: Dr Michael Drivas
Clinic: Bankstown Specialist in Broken Bones
Address : 71 Meredith street
VC001 College of Sports & Fitness - 11/05/2017- SISFFIT015
International College of Capoeira Pty Ltd trading as ’College of Sports & Fitness’ ABN 90 125 114 730/ Registered
Training Organisation 91345/ CRICOS Provider Code 03057C
some early rounds of physiotherapy. Peter’s doctor has recommended that he start going to the gym
to get fit and healthy again. Prior to his motor vehicle accident Peter walked daily, but he has never
exercised in a gym before. Peter reports feeling very tight in the calf muscles and ankle since the
plaster was removed six weeks ago. Peter’s other health information, as provided by his doctor,
includes:
● a blood pressure reading of 142/92 bpm
● asthma (he takes ventolin)
● poor eating habits, such as frequent takeaway lunches at work and dinner, skipping breakfast.
Note: Although this doctor has suggested that Peter join a gym, you should still assume that you will
require clearance from the relevant medical and/or allied health professionals prior to exercise
testing and/or programming when considering Peter’s medical and health status.
Referral letter from Health ProfessionaL TO Fitness Trainer
Practitioner Name: Dr Michael Drivas
Clinic: Bankstown Specialist in Broken Bones
Address : 71 Meredith street
VC001 College of Sports & Fitness - 11/05/2017- SISFFIT015
International College of Capoeira Pty Ltd trading as ’College of Sports & Fitness’ ABN 90 125 114 730/ Registered
Training Organisation 91345/ CRICOS Provider Code 03057C
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Assessment 1- Portfolio (SISSFFIT015)
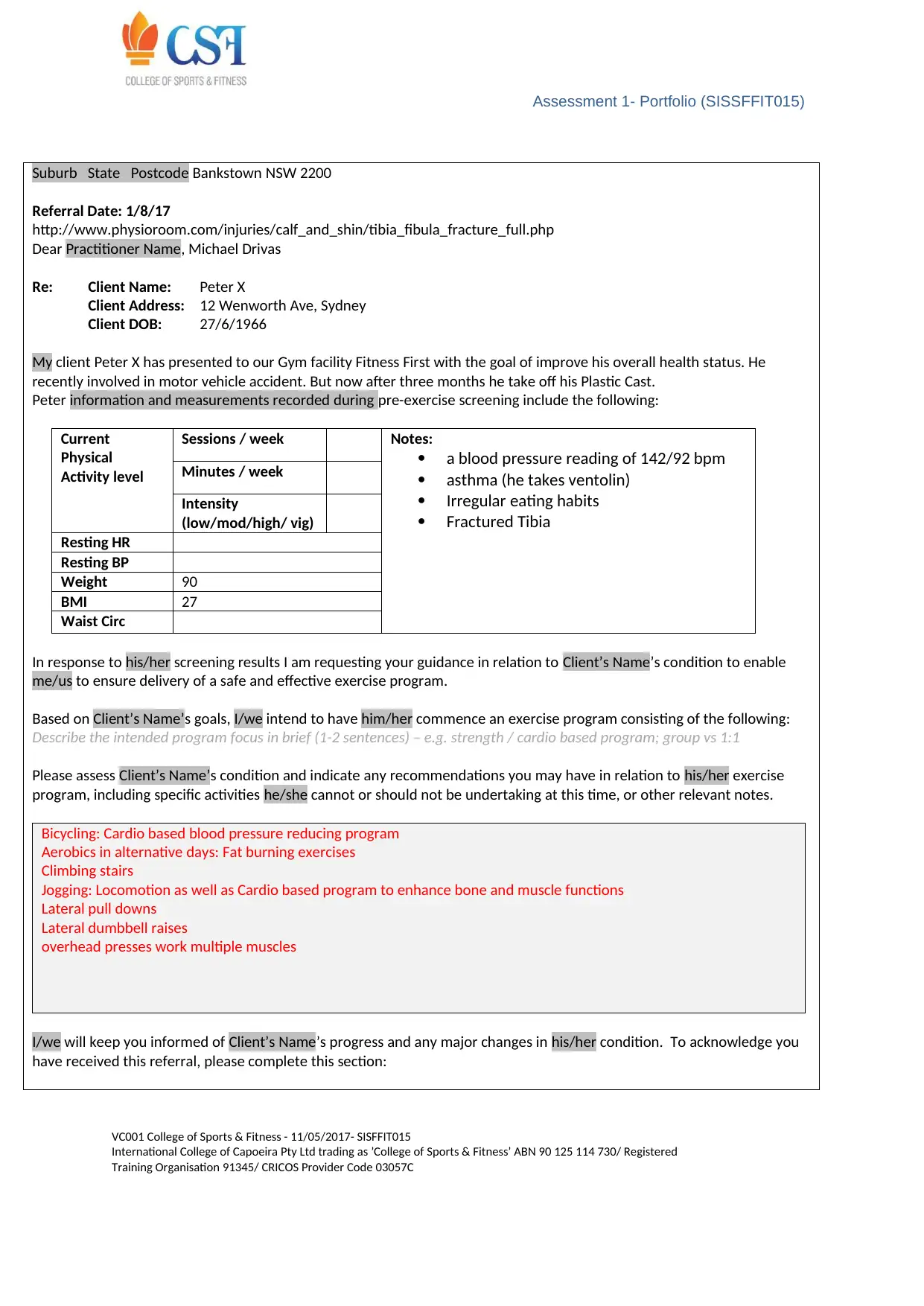
Suburb State Postcode Bankstown NSW 2200
Referral Date: 1/8/17
http://www.physioroom.com/injuries/calf_and_shin/tibia_fibula_fracture_full.php
Dear Practitioner Name, Michael Drivas
Re: Client Name: Peter X
Client Address: 12 Wenworth Ave, Sydney
Client DOB: 27/6/1966
My client Peter X has presented to our Gym facility Fitness First with the goal of improve his overall health status. He
recently involved in motor vehicle accident. But now after three months he take off his Plastic Cast.
Peter information and measurements recorded during pre-exercise screening include the following:
Current
Physical
Activity level
Sessions / week Notes:
a blood pressure reading of 142/92 bpm
asthma (he takes ventolin)
Irregular eating habits
Fractured Tibia
Minutes / week
Intensity
(low/mod/high/ vig)
Resting HR
Resting BP
Weight 90
BMI 27
Waist Circ
In response to his/her screening results I am requesting your guidance in relation to Client’s Name’s condition to enable
me/us to ensure delivery of a safe and effective exercise program.
Based on Client’s Name’s goals, I/we intend to have him/her commence an exercise program consisting of the following:
Describe the intended program focus in brief (1-2 sentences) – e.g. strength / cardio based program; group vs 1:1
Please assess Client’s Name’s condition and indicate any recommendations you may have in relation to his/her exercise
program, including specific activities he/she cannot or should not be undertaking at this time, or other relevant notes.
Bicycling: Cardio based blood pressure reducing program
Aerobics in alternative days: Fat burning exercises
Climbing stairs
Jogging: Locomotion as well as Cardio based program to enhance bone and muscle functions
Lateral pull downs
Lateral dumbbell raises
overhead presses work multiple muscles
I/we will keep you informed of Client’s Name’s progress and any major changes in his/her condition. To acknowledge you
have received this referral, please complete this section:
VC001 College of Sports & Fitness - 11/05/2017- SISFFIT015
International College of Capoeira Pty Ltd trading as ’College of Sports & Fitness’ ABN 90 125 114 730/ Registered
Training Organisation 91345/ CRICOS Provider Code 03057C
Suburb State Postcode Bankstown NSW 2200
Referral Date: 1/8/17
http://www.physioroom.com/injuries/calf_and_shin/tibia_fibula_fracture_full.php
Dear Practitioner Name, Michael Drivas
Re: Client Name: Peter X
Client Address: 12 Wenworth Ave, Sydney
Client DOB: 27/6/1966
My client Peter X has presented to our Gym facility Fitness First with the goal of improve his overall health status. He
recently involved in motor vehicle accident. But now after three months he take off his Plastic Cast.
Peter information and measurements recorded during pre-exercise screening include the following:
Current
Physical
Activity level
Sessions / week Notes:
a blood pressure reading of 142/92 bpm
asthma (he takes ventolin)
Irregular eating habits
Fractured Tibia
Minutes / week
Intensity
(low/mod/high/ vig)
Resting HR
Resting BP
Weight 90
BMI 27
Waist Circ
In response to his/her screening results I am requesting your guidance in relation to Client’s Name’s condition to enable
me/us to ensure delivery of a safe and effective exercise program.
Based on Client’s Name’s goals, I/we intend to have him/her commence an exercise program consisting of the following:
Describe the intended program focus in brief (1-2 sentences) – e.g. strength / cardio based program; group vs 1:1
Please assess Client’s Name’s condition and indicate any recommendations you may have in relation to his/her exercise
program, including specific activities he/she cannot or should not be undertaking at this time, or other relevant notes.
Bicycling: Cardio based blood pressure reducing program
Aerobics in alternative days: Fat burning exercises
Climbing stairs
Jogging: Locomotion as well as Cardio based program to enhance bone and muscle functions
Lateral pull downs
Lateral dumbbell raises
overhead presses work multiple muscles
I/we will keep you informed of Client’s Name’s progress and any major changes in his/her condition. To acknowledge you
have received this referral, please complete this section:
VC001 College of Sports & Fitness - 11/05/2017- SISFFIT015
International College of Capoeira Pty Ltd trading as ’College of Sports & Fitness’ ABN 90 125 114 730/ Registered
Training Organisation 91345/ CRICOS Provider Code 03057C
Assessment 1- Portfolio (SISSFFIT015)
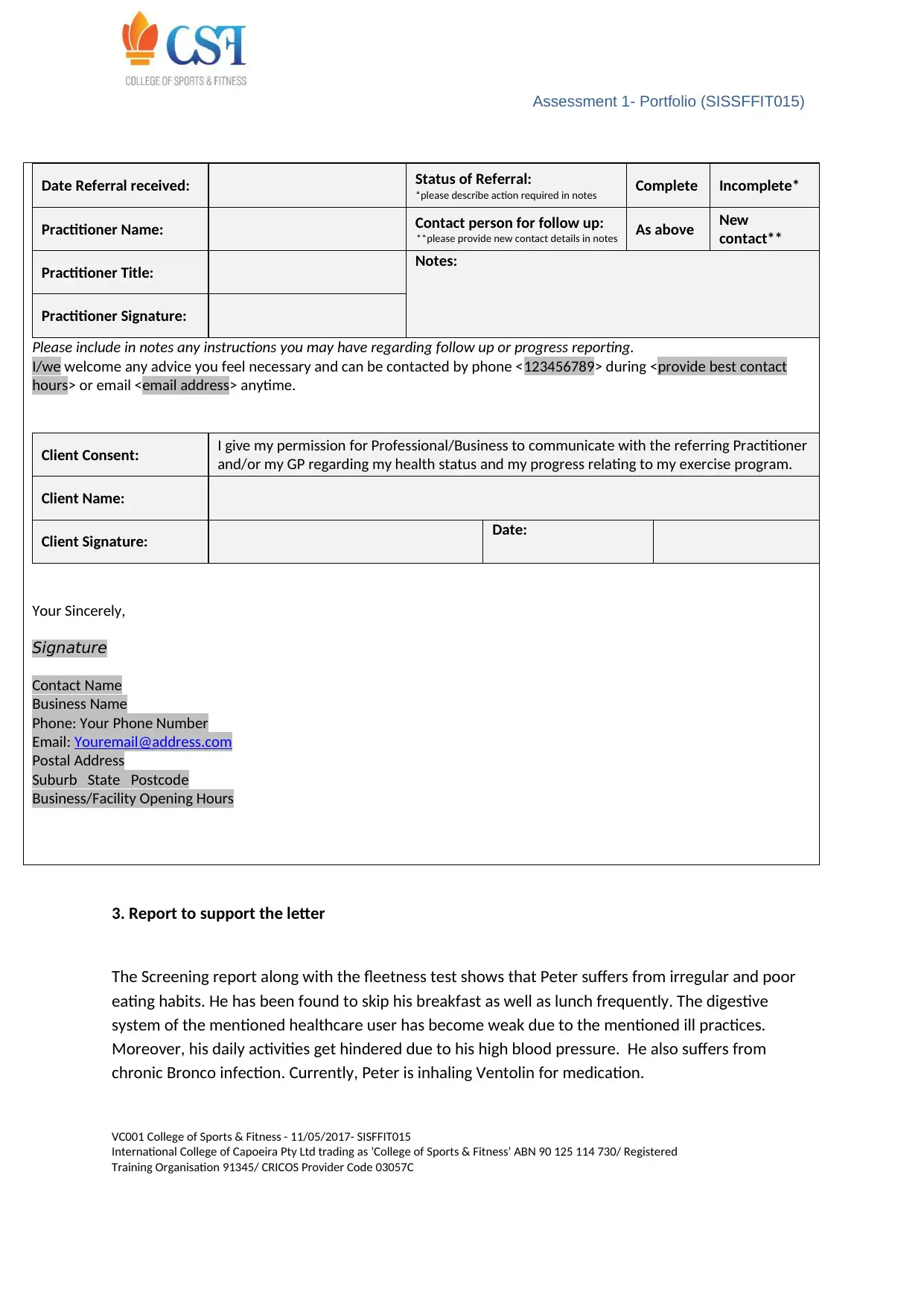
Date Referral received: Status of Referral:
*please describe action required in notes Complete Incomplete*
Practitioner Name: Contact person for follow up:
**please provide new contact details in notes As above New
contact**
Practitioner Title: Notes:
Practitioner Signature:
Please include in notes any instructions you may have regarding follow up or progress reporting.
I/we welcome any advice you feel necessary and can be contacted by phone <123456789> during <provide best contact
hours> or email <email address> anytime.
Client Consent: I give my permission for Professional/Business to communicate with the referring Practitioner
and/or my GP regarding my health status and my progress relating to my exercise program.
Client Name:
Client Signature: Date:
Your Sincerely,
Signature
Contact Name
Business Name
Phone: Your Phone Number
Email: Youremail@address.com
Postal Address
Suburb State Postcode
Business/Facility Opening Hours
3. Report to support the letter
The Screening report along with the fleetness test shows that Peter suffers from irregular and poor
eating habits. He has been found to skip his breakfast as well as lunch frequently. The digestive
system of the mentioned healthcare user has become weak due to the mentioned ill practices.
Moreover, his daily activities get hindered due to his high blood pressure. He also suffers from
chronic Bronco infection. Currently, Peter is inhaling Ventolin for medication.
VC001 College of Sports & Fitness - 11/05/2017- SISFFIT015
International College of Capoeira Pty Ltd trading as ’College of Sports & Fitness’ ABN 90 125 114 730/ Registered
Training Organisation 91345/ CRICOS Provider Code 03057C
Date Referral received: Status of Referral:
*please describe action required in notes Complete Incomplete*
Practitioner Name: Contact person for follow up:
**please provide new contact details in notes As above New
contact**
Practitioner Title: Notes:
Practitioner Signature:
Please include in notes any instructions you may have regarding follow up or progress reporting.
I/we welcome any advice you feel necessary and can be contacted by phone <123456789> during <provide best contact
hours> or email <email address> anytime.
Client Consent: I give my permission for Professional/Business to communicate with the referring Practitioner
and/or my GP regarding my health status and my progress relating to my exercise program.
Client Name:
Client Signature: Date:
Your Sincerely,
Signature
Contact Name
Business Name
Phone: Your Phone Number
Email: Youremail@address.com
Postal Address
Suburb State Postcode
Business/Facility Opening Hours
3. Report to support the letter
The Screening report along with the fleetness test shows that Peter suffers from irregular and poor
eating habits. He has been found to skip his breakfast as well as lunch frequently. The digestive
system of the mentioned healthcare user has become weak due to the mentioned ill practices.
Moreover, his daily activities get hindered due to his high blood pressure. He also suffers from
chronic Bronco infection. Currently, Peter is inhaling Ventolin for medication.
VC001 College of Sports & Fitness - 11/05/2017- SISFFIT015
International College of Capoeira Pty Ltd trading as ’College of Sports & Fitness’ ABN 90 125 114 730/ Registered
Training Organisation 91345/ CRICOS Provider Code 03057C
Assessment 1- Portfolio (SISSFFIT015)
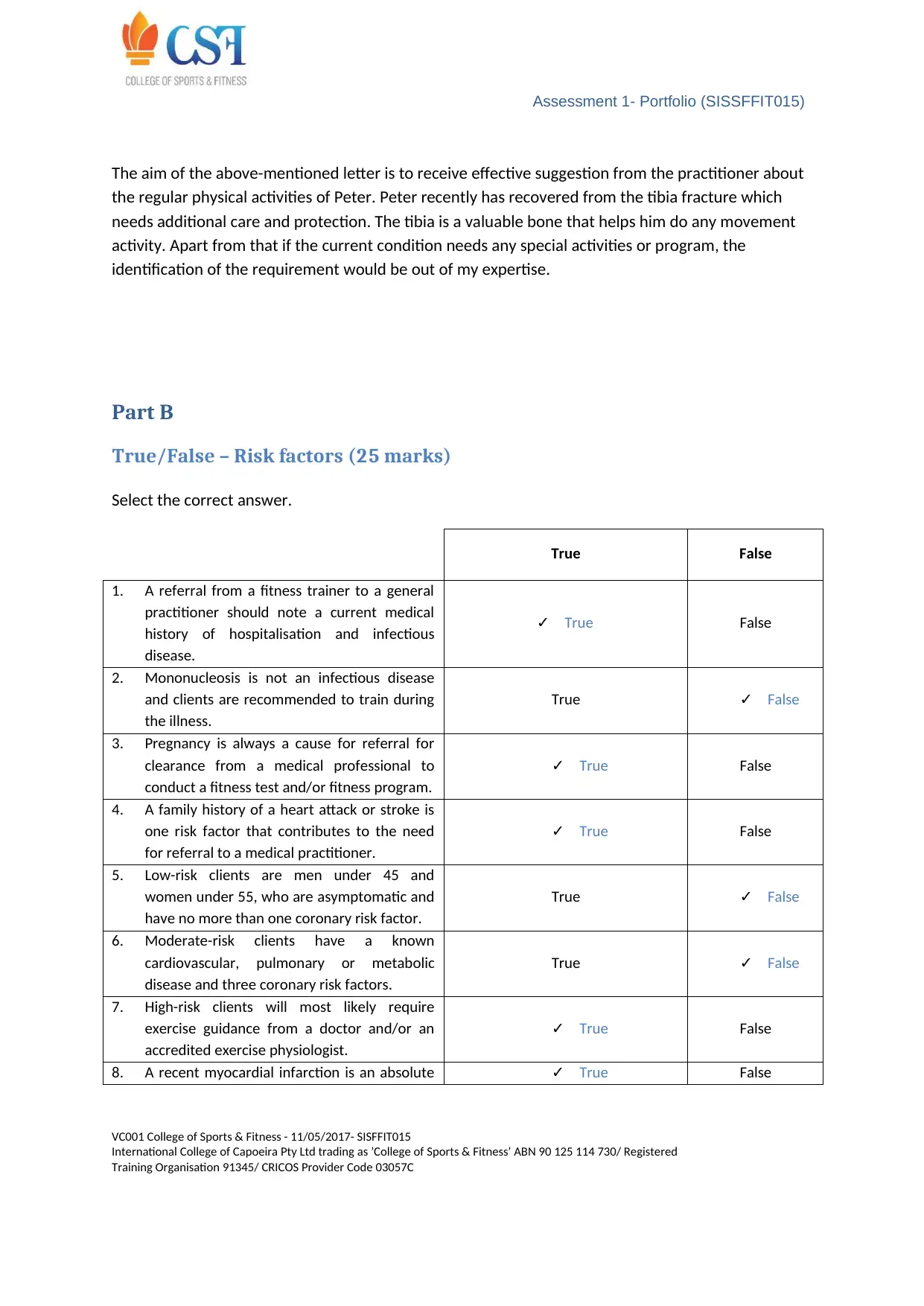
The aim of the above-mentioned letter is to receive effective suggestion from the practitioner about
the regular physical activities of Peter. Peter recently has recovered from the tibia fracture which
needs additional care and protection. The tibia is a valuable bone that helps him do any movement
activity. Apart from that if the current condition needs any special activities or program, the
identification of the requirement would be out of my expertise.
Part B
True/False – Risk factors (25 marks)
Select the correct answer.
True False
1. A referral from a fitness trainer to a general
practitioner should note a current medical
history of hospitalisation and infectious
disease.
✓ True False
2. Mononucleosis is not an infectious disease
and clients are recommended to train during
the illness.
True ✓ False
3. Pregnancy is always a cause for referral for
clearance from a medical professional to
conduct a fitness test and/or fitness program.
✓ True False
4. A family history of a heart attack or stroke is
one risk factor that contributes to the need
for referral to a medical practitioner.
✓ True False
5. Low-risk clients are men under 45 and
women under 55, who are asymptomatic and
have no more than one coronary risk factor.
True ✓ False
6. Moderate-risk clients have a known
cardiovascular, pulmonary or metabolic
disease and three coronary risk factors.
True ✓ False
7. High-risk clients will most likely require
exercise guidance from a doctor and/or an
accredited exercise physiologist.
✓ True False
8. A recent myocardial infarction is an absolute ✓ True False
VC001 College of Sports & Fitness - 11/05/2017- SISFFIT015
International College of Capoeira Pty Ltd trading as ’College of Sports & Fitness’ ABN 90 125 114 730/ Registered
Training Organisation 91345/ CRICOS Provider Code 03057C
The aim of the above-mentioned letter is to receive effective suggestion from the practitioner about
the regular physical activities of Peter. Peter recently has recovered from the tibia fracture which
needs additional care and protection. The tibia is a valuable bone that helps him do any movement
activity. Apart from that if the current condition needs any special activities or program, the
identification of the requirement would be out of my expertise.
Part B
True/False – Risk factors (25 marks)
Select the correct answer.
True False
1. A referral from a fitness trainer to a general
practitioner should note a current medical
history of hospitalisation and infectious
disease.
✓ True False
2. Mononucleosis is not an infectious disease
and clients are recommended to train during
the illness.
True ✓ False
3. Pregnancy is always a cause for referral for
clearance from a medical professional to
conduct a fitness test and/or fitness program.
✓ True False
4. A family history of a heart attack or stroke is
one risk factor that contributes to the need
for referral to a medical practitioner.
✓ True False
5. Low-risk clients are men under 45 and
women under 55, who are asymptomatic and
have no more than one coronary risk factor.
True ✓ False
6. Moderate-risk clients have a known
cardiovascular, pulmonary or metabolic
disease and three coronary risk factors.
True ✓ False
7. High-risk clients will most likely require
exercise guidance from a doctor and/or an
accredited exercise physiologist.
✓ True False
8. A recent myocardial infarction is an absolute ✓ True False
VC001 College of Sports & Fitness - 11/05/2017- SISFFIT015
International College of Capoeira Pty Ltd trading as ’College of Sports & Fitness’ ABN 90 125 114 730/ Registered
Training Organisation 91345/ CRICOS Provider Code 03057C
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Assessment 1- Portfolio (SISSFFIT015)
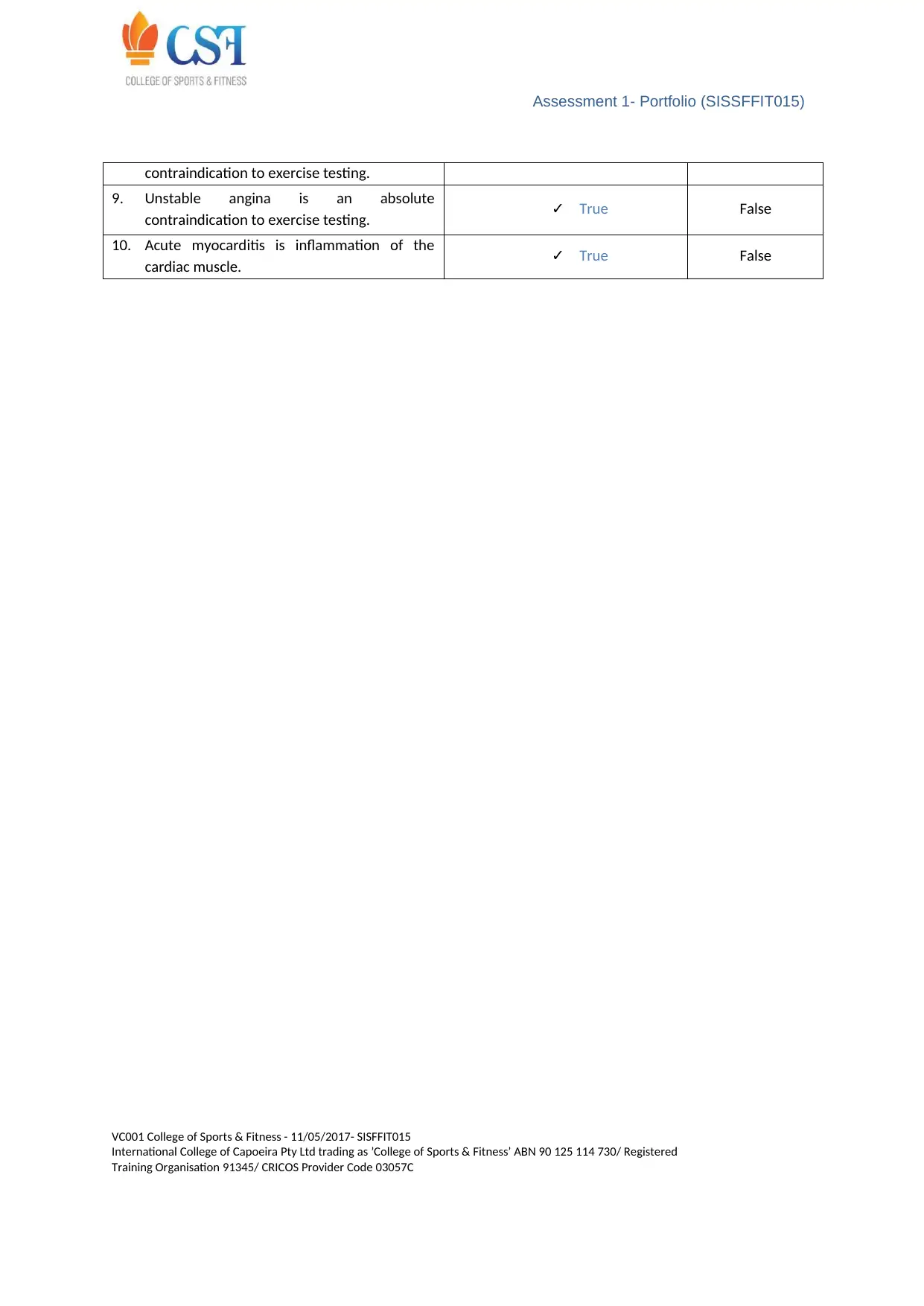
contraindication to exercise testing.
9. Unstable angina is an absolute
contraindication to exercise testing. ✓ True False
10. Acute myocarditis is inflammation of the
cardiac muscle. ✓ True False
VC001 College of Sports & Fitness - 11/05/2017- SISFFIT015
International College of Capoeira Pty Ltd trading as ’College of Sports & Fitness’ ABN 90 125 114 730/ Registered
Training Organisation 91345/ CRICOS Provider Code 03057C
contraindication to exercise testing.
9. Unstable angina is an absolute
contraindication to exercise testing. ✓ True False
10. Acute myocarditis is inflammation of the
cardiac muscle. ✓ True False
VC001 College of Sports & Fitness - 11/05/2017- SISFFIT015
International College of Capoeira Pty Ltd trading as ’College of Sports & Fitness’ ABN 90 125 114 730/ Registered
Training Organisation 91345/ CRICOS Provider Code 03057C
Assessment 1- Portfolio (SISSFFIT015)
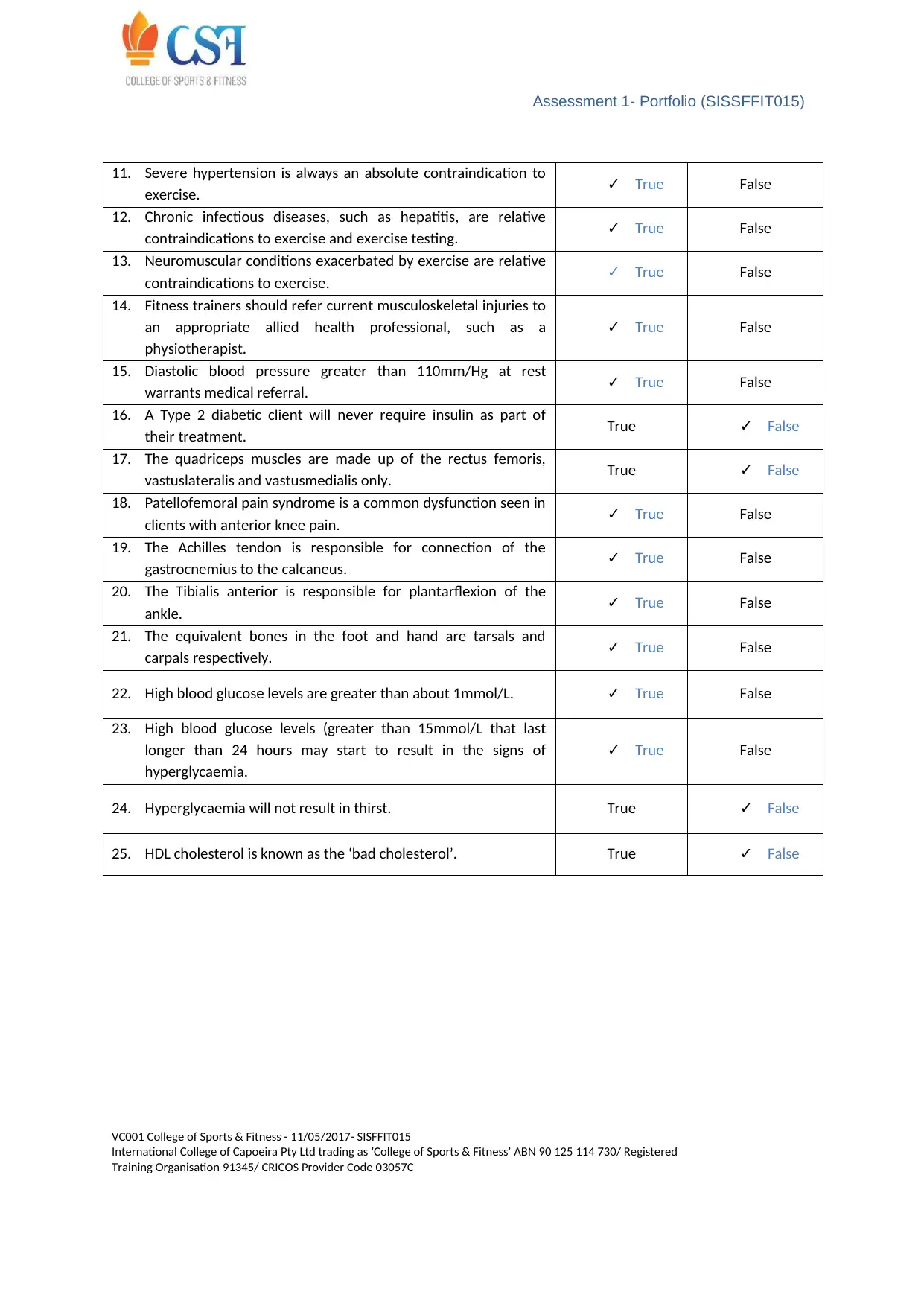
11. Severe hypertension is always an absolute contraindication to
exercise. ✓ True False
12. Chronic infectious diseases, such as hepatitis, are relative
contraindications to exercise and exercise testing. ✓ True False
13. Neuromuscular conditions exacerbated by exercise are relative
contraindications to exercise. ✓ True False
14. Fitness trainers should refer current musculoskeletal injuries to
an appropriate allied health professional, such as a
physiotherapist.
✓ True False
15. Diastolic blood pressure greater than 110mm/Hg at rest
warrants medical referral. ✓ True False
16. A Type 2 diabetic client will never require insulin as part of
their treatment. True ✓ False
17. The quadriceps muscles are made up of the rectus femoris,
vastuslateralis and vastusmedialis only. True ✓ False
18. Patellofemoral pain syndrome is a common dysfunction seen in
clients with anterior knee pain. ✓ True False
19. The Achilles tendon is responsible for connection of the
gastrocnemius to the calcaneus. ✓ True False
20. The Tibialis anterior is responsible for plantarflexion of the
ankle. ✓ True False
21. The equivalent bones in the foot and hand are tarsals and
carpals respectively. ✓ True False
22. High blood glucose levels are greater than about 1mmol/L. ✓ True False
23. High blood glucose levels (greater than 15mmol/L that last
longer than 24 hours may start to result in the signs of
hyperglycaemia.
✓ True False
24. Hyperglycaemia will not result in thirst. True ✓ False
25. HDL cholesterol is known as the ‘bad cholesterol’. True ✓ False
VC001 College of Sports & Fitness - 11/05/2017- SISFFIT015
International College of Capoeira Pty Ltd trading as ’College of Sports & Fitness’ ABN 90 125 114 730/ Registered
Training Organisation 91345/ CRICOS Provider Code 03057C
11. Severe hypertension is always an absolute contraindication to
exercise. ✓ True False
12. Chronic infectious diseases, such as hepatitis, are relative
contraindications to exercise and exercise testing. ✓ True False
13. Neuromuscular conditions exacerbated by exercise are relative
contraindications to exercise. ✓ True False
14. Fitness trainers should refer current musculoskeletal injuries to
an appropriate allied health professional, such as a
physiotherapist.
✓ True False
15. Diastolic blood pressure greater than 110mm/Hg at rest
warrants medical referral. ✓ True False
16. A Type 2 diabetic client will never require insulin as part of
their treatment. True ✓ False
17. The quadriceps muscles are made up of the rectus femoris,
vastuslateralis and vastusmedialis only. True ✓ False
18. Patellofemoral pain syndrome is a common dysfunction seen in
clients with anterior knee pain. ✓ True False
19. The Achilles tendon is responsible for connection of the
gastrocnemius to the calcaneus. ✓ True False
20. The Tibialis anterior is responsible for plantarflexion of the
ankle. ✓ True False
21. The equivalent bones in the foot and hand are tarsals and
carpals respectively. ✓ True False
22. High blood glucose levels are greater than about 1mmol/L. ✓ True False
23. High blood glucose levels (greater than 15mmol/L that last
longer than 24 hours may start to result in the signs of
hyperglycaemia.
✓ True False
24. Hyperglycaemia will not result in thirst. True ✓ False
25. HDL cholesterol is known as the ‘bad cholesterol’. True ✓ False
VC001 College of Sports & Fitness - 11/05/2017- SISFFIT015
International College of Capoeira Pty Ltd trading as ’College of Sports & Fitness’ ABN 90 125 114 730/ Registered
Training Organisation 91345/ CRICOS Provider Code 03057C
Assessment 1- Portfolio (SISSFFIT015)
Part C
Case study – Referral (15 marks)
This task involves the receiving of simulated referrals from medical and allied health professionals
and making decisions as to what plan of action you might take in response to each referral. Each
referral situation is provided as a case study.
Katherine X
Dr Jones is a local general practitioner. He has referred Katherine to you (as a fitness trainer)
because he would like her to start exercising. Katherine is obese, reporting poor dietary habits, and
has Type 2 diabetes. Her resting blood pressure is 145/91mmHg. Katherine has arrived at the gym to
buy a membership based on Dr Jones ‘telling me to come and see you’. The referral letter is as
follows:
Dear Sir/Madam,
Katherine X is a 57-year-old female patient who has recently been diagnosed with Type 2 diabetes.
Katherine is still learning about this condition and would benefit from further education and lifestyle
modification. Her blood pressure is 145/91mmHg and she has commenced medication to assist in
this being reduced. She will need an exercise program to assist with management of her condition.
She is 89kg and 168cm tall.
Regards,
Dr Jones.
VC001 College of Sports & Fitness - 11/05/2017- SISFFIT015
International College of Capoeira Pty Ltd trading as ’College of Sports & Fitness’ ABN 90 125 114 730/ Registered
Training Organisation 91345/ CRICOS Provider Code 03057C
Part C
Case study – Referral (15 marks)
This task involves the receiving of simulated referrals from medical and allied health professionals
and making decisions as to what plan of action you might take in response to each referral. Each
referral situation is provided as a case study.
Katherine X
Dr Jones is a local general practitioner. He has referred Katherine to you (as a fitness trainer)
because he would like her to start exercising. Katherine is obese, reporting poor dietary habits, and
has Type 2 diabetes. Her resting blood pressure is 145/91mmHg. Katherine has arrived at the gym to
buy a membership based on Dr Jones ‘telling me to come and see you’. The referral letter is as
follows:
Dear Sir/Madam,
Katherine X is a 57-year-old female patient who has recently been diagnosed with Type 2 diabetes.
Katherine is still learning about this condition and would benefit from further education and lifestyle
modification. Her blood pressure is 145/91mmHg and she has commenced medication to assist in
this being reduced. She will need an exercise program to assist with management of her condition.
She is 89kg and 168cm tall.
Regards,
Dr Jones.
VC001 College of Sports & Fitness - 11/05/2017- SISFFIT015
International College of Capoeira Pty Ltd trading as ’College of Sports & Fitness’ ABN 90 125 114 730/ Registered
Training Organisation 91345/ CRICOS Provider Code 03057C
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Assessment 1- Portfolio (SISSFFIT015)
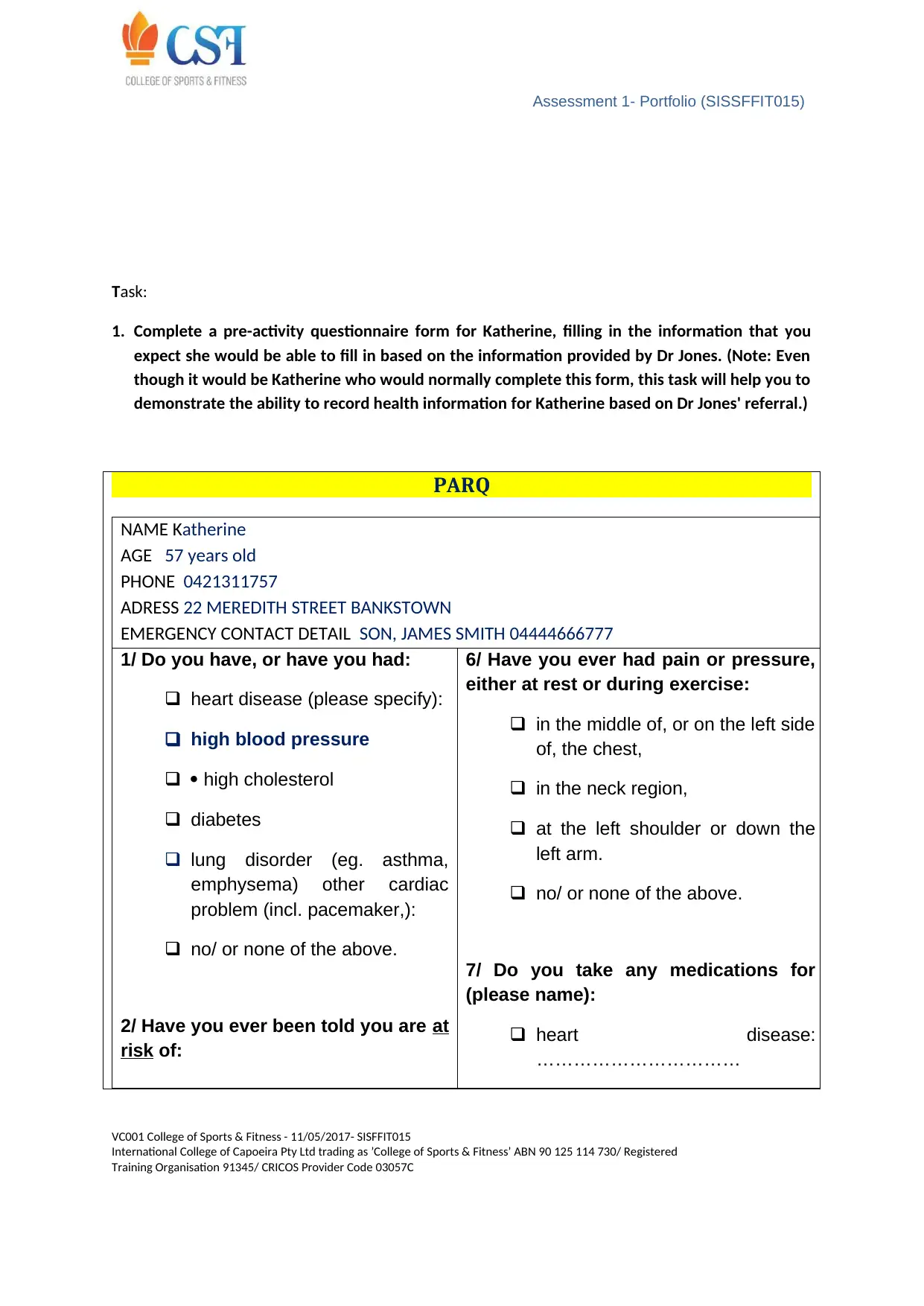
Task:
1. Complete a pre-activity questionnaire form for Katherine, filling in the information that you
expect she would be able to fill in based on the information provided by Dr Jones. (Note: Even
though it would be Katherine who would normally complete this form, this task will help you to
demonstrate the ability to record health information for Katherine based on Dr Jones' referral.)
PARQ
NAME Katherine
AGE 57 years old
PHONE 0421311757
ADRESS 22 MEREDITH STREET BANKSTOWN
EMERGENCY CONTACT DETAIL SON, JAMES SMITH 04444666777
1/ Do you have, or have you had:
heart disease (please specify):
high blood pressure
high cholesterol
diabetes
lung disorder (eg. asthma,
emphysema) other cardiac
problem (incl. pacemaker,):
no/ or none of the above.
2/ Have you ever been told you are at
risk of:
6/ Have you ever had pain or pressure,
either at rest or during exercise:
in the middle of, or on the left side
of, the chest,
in the neck region,
at the left shoulder or down the
left arm.
no/ or none of the above.
7/ Do you take any medications for
(please name):
heart disease:
……………………………
VC001 College of Sports & Fitness - 11/05/2017- SISFFIT015
International College of Capoeira Pty Ltd trading as ’College of Sports & Fitness’ ABN 90 125 114 730/ Registered
Training Organisation 91345/ CRICOS Provider Code 03057C
Task:
1. Complete a pre-activity questionnaire form for Katherine, filling in the information that you
expect she would be able to fill in based on the information provided by Dr Jones. (Note: Even
though it would be Katherine who would normally complete this form, this task will help you to
demonstrate the ability to record health information for Katherine based on Dr Jones' referral.)
PARQ
NAME Katherine
AGE 57 years old
PHONE 0421311757
ADRESS 22 MEREDITH STREET BANKSTOWN
EMERGENCY CONTACT DETAIL SON, JAMES SMITH 04444666777
1/ Do you have, or have you had:
heart disease (please specify):
high blood pressure
high cholesterol
diabetes
lung disorder (eg. asthma,
emphysema) other cardiac
problem (incl. pacemaker,):
no/ or none of the above.
2/ Have you ever been told you are at
risk of:
6/ Have you ever had pain or pressure,
either at rest or during exercise:
in the middle of, or on the left side
of, the chest,
in the neck region,
at the left shoulder or down the
left arm.
no/ or none of the above.
7/ Do you take any medications for
(please name):
heart disease:
……………………………
VC001 College of Sports & Fitness - 11/05/2017- SISFFIT015
International College of Capoeira Pty Ltd trading as ’College of Sports & Fitness’ ABN 90 125 114 730/ Registered
Training Organisation 91345/ CRICOS Provider Code 03057C
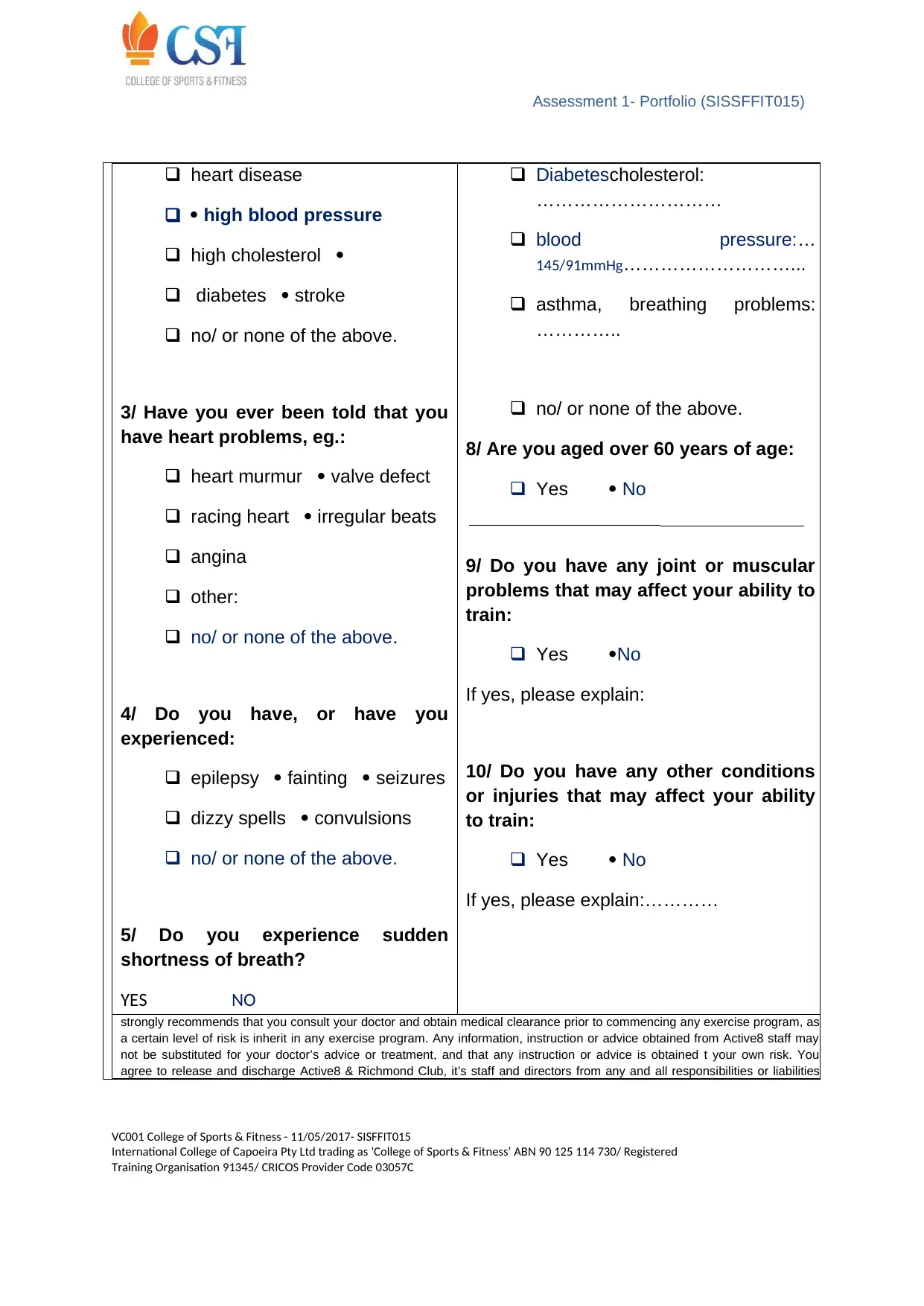
Assessment 1- Portfolio (SISSFFIT015)
heart disease
high blood pressure
high cholesterol
diabetes stroke
no/ or none of the above.
3/ Have you ever been told that you
have heart problems, eg.:
heart murmur valve defect
racing heart irregular beats
angina
other:
no/ or none of the above.
4/ Do you have, or have you
experienced:
epilepsy fainting seizures
dizzy spells convulsions
no/ or none of the above.
5/ Do you experience sudden
shortness of breath?
YES NO
Diabetescholesterol:
…………………………
blood pressure:…
145/91mmHg………………………...
asthma, breathing problems:
…………..
no/ or none of the above.
8/ Are you aged over 60 years of age:
Yes No
9/ Do you have any joint or muscular
problems that may affect your ability to
train:
Yes No
If yes, please explain:
10/ Do you have any other conditions
or injuries that may affect your ability
to train:
Yes No
If yes, please explain:…………
strongly recommends that you consult your doctor and obtain medical clearance prior to commencing any exercise program, as
a certain level of risk is inherit in any exercise program. Any information, instruction or advice obtained from Active8 staff may
not be substituted for your doctor’s advice or treatment, and that any instruction or advice is obtained t your own risk. You
agree to release and discharge Active8 & Richmond Club, it’s staff and directors from any and all responsibilities or liabilities
VC001 College of Sports & Fitness - 11/05/2017- SISFFIT015
International College of Capoeira Pty Ltd trading as ’College of Sports & Fitness’ ABN 90 125 114 730/ Registered
Training Organisation 91345/ CRICOS Provider Code 03057C
heart disease
high blood pressure
high cholesterol
diabetes stroke
no/ or none of the above.
3/ Have you ever been told that you
have heart problems, eg.:
heart murmur valve defect
racing heart irregular beats
angina
other:
no/ or none of the above.
4/ Do you have, or have you
experienced:
epilepsy fainting seizures
dizzy spells convulsions
no/ or none of the above.
5/ Do you experience sudden
shortness of breath?
YES NO
Diabetescholesterol:
…………………………
blood pressure:…
145/91mmHg………………………...
asthma, breathing problems:
…………..
no/ or none of the above.
8/ Are you aged over 60 years of age:
Yes No
9/ Do you have any joint or muscular
problems that may affect your ability to
train:
Yes No
If yes, please explain:
10/ Do you have any other conditions
or injuries that may affect your ability
to train:
Yes No
If yes, please explain:…………
strongly recommends that you consult your doctor and obtain medical clearance prior to commencing any exercise program, as
a certain level of risk is inherit in any exercise program. Any information, instruction or advice obtained from Active8 staff may
not be substituted for your doctor’s advice or treatment, and that any instruction or advice is obtained t your own risk. You
agree to release and discharge Active8 & Richmond Club, it’s staff and directors from any and all responsibilities or liabilities
VC001 College of Sports & Fitness - 11/05/2017- SISFFIT015
International College of Capoeira Pty Ltd trading as ’College of Sports & Fitness’ ABN 90 125 114 730/ Registered
Training Organisation 91345/ CRICOS Provider Code 03057C
Assessment 1- Portfolio (SISSFFIT015)
from injury or illness arising from your participation in any activity undertake at Active8 or upon our advice.
Administration Only - Referral to Medical Practitioner required?
Client is: aged 18-60 and has no risk factors >>> cleared for moderate exercise
prescription
Client responded to one or more of Cardio-Respiratory risks >>> refer to Doctor for clearance
Signatures: Client:KATHERINE Staff : ..MARIANNA SOFIANIDOU..... Date: …16/5/18.
2. Write a short report (approximately 500–750 words) outlining:
a) Katherine’s risk factors, including calculation of her BMI for poor health
Obese ,poor eating habits, has Type 2 Diabetes,High blood pressure 145/91mmHg which must
reduced for this reason she getting medication
b) the relevance of BMI in this situation
She is 89kg and 168cm tall
BMI 31.5 - Obese
c) a suggested management plan for Katherine
Katherine is obese patient that must as soon as possible lose weight for her healthier future. The
benefits she will get is not only to how she gonna feel but she will reduce all this risk factors
she already has,such as Type 2 Diabetes. Also by reducing weight she will reduce her future
problem with bones and joints and reduce risk of future cancer.She must reduce the amount
of intakes she gets daily and exercising almost 4 days a week. Her BMI must range between
20-25 as per high and must be loose about 17 kg to reach approxematly 70 kg recommend for
her high
d) what guidance you will require from medical and/or allied health professionals prior to
fitness testing and/or fitness programming for Katherine.
Client’s risk and needs
VC001 College of Sports & Fitness - 11/05/2017- SISFFIT015
International College of Capoeira Pty Ltd trading as ’College of Sports & Fitness’ ABN 90 125 114 730/ Registered
Training Organisation 91345/ CRICOS Provider Code 03057C
from injury or illness arising from your participation in any activity undertake at Active8 or upon our advice.
Administration Only - Referral to Medical Practitioner required?
Client is: aged 18-60 and has no risk factors >>> cleared for moderate exercise
prescription
Client responded to one or more of Cardio-Respiratory risks >>> refer to Doctor for clearance
Signatures: Client:KATHERINE Staff : ..MARIANNA SOFIANIDOU..... Date: …16/5/18.
2. Write a short report (approximately 500–750 words) outlining:
a) Katherine’s risk factors, including calculation of her BMI for poor health
Obese ,poor eating habits, has Type 2 Diabetes,High blood pressure 145/91mmHg which must
reduced for this reason she getting medication
b) the relevance of BMI in this situation
She is 89kg and 168cm tall
BMI 31.5 - Obese
c) a suggested management plan for Katherine
Katherine is obese patient that must as soon as possible lose weight for her healthier future. The
benefits she will get is not only to how she gonna feel but she will reduce all this risk factors
she already has,such as Type 2 Diabetes. Also by reducing weight she will reduce her future
problem with bones and joints and reduce risk of future cancer.She must reduce the amount
of intakes she gets daily and exercising almost 4 days a week. Her BMI must range between
20-25 as per high and must be loose about 17 kg to reach approxematly 70 kg recommend for
her high
d) what guidance you will require from medical and/or allied health professionals prior to
fitness testing and/or fitness programming for Katherine.
Client’s risk and needs
VC001 College of Sports & Fitness - 11/05/2017- SISFFIT015
International College of Capoeira Pty Ltd trading as ’College of Sports & Fitness’ ABN 90 125 114 730/ Registered
Training Organisation 91345/ CRICOS Provider Code 03057C
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Assessment 1- Portfolio (SISSFFIT015)
Katherine suffers from good number risk factors that include obesity, poor eating habits, high blood
pressuring and Type 2 diabetes. This high weight is causing high blood pressure as well. If needed
this high blood pressure of 145/91mmHg has to be cured with appropriate medication and other
treatment.
Exercise type
Bicycling: Cardio based blood pressure reducing program
Aerobics in alternative days: Fat burning exercises
Climbing stairs
Jogging: Locomotion as well as Cardio based program to enhance bone and muscle functions
Lateral pull downs
Lateral dumbbell raises
overhead presses work multiple muscles
3. Write referral letters for medical and/or allied health professionals in your local area that you
might suggest that Katherine should see either before or during your time with her. Ensure you
provide a rationale for your referral.
Practitioner Name KATE HOLMES
ClinicINGRID ORTH DIETITIAN AND NUTRITIONIST
Suburb BANKSTOWN State NSW Postcode 2200
Referral Date: 16/5/18
Dear Mr HOLMES
Re: Client Name: KATHERINE
Client Address: BANKSTOWN
Client DOB: 57 YEARS OLD
MY client KATHERINE X has presented to our business/service/facility with the goal of lose weight as her GP suggest she
must exercise to reduce her health risk factors such as Type 2 Diabetes
KATHERINEinformation and measurements recorded during pre-exercise screening include the following:
Current
Physical
Activity level
NOT AT ALL
Sessions / week Notes:
─ TYPE 2 DIABETES
─ BMI -OBESITY
─ HIGH BLOOD PRESSURE 145/91mmHg
─ UNDER MEDICATION
─
Minutes / week
Intensity
(low/mod/high/ vig)
Resting HR
Resting BP
Weight
VC001 College of Sports & Fitness - 11/05/2017- SISFFIT015
International College of Capoeira Pty Ltd trading as ’College of Sports & Fitness’ ABN 90 125 114 730/ Registered
Training Organisation 91345/ CRICOS Provider Code 03057C
Katherine suffers from good number risk factors that include obesity, poor eating habits, high blood
pressuring and Type 2 diabetes. This high weight is causing high blood pressure as well. If needed
this high blood pressure of 145/91mmHg has to be cured with appropriate medication and other
treatment.
Exercise type
Bicycling: Cardio based blood pressure reducing program
Aerobics in alternative days: Fat burning exercises
Climbing stairs
Jogging: Locomotion as well as Cardio based program to enhance bone and muscle functions
Lateral pull downs
Lateral dumbbell raises
overhead presses work multiple muscles
3. Write referral letters for medical and/or allied health professionals in your local area that you
might suggest that Katherine should see either before or during your time with her. Ensure you
provide a rationale for your referral.
Practitioner Name KATE HOLMES
ClinicINGRID ORTH DIETITIAN AND NUTRITIONIST
Suburb BANKSTOWN State NSW Postcode 2200
Referral Date: 16/5/18
Dear Mr HOLMES
Re: Client Name: KATHERINE
Client Address: BANKSTOWN
Client DOB: 57 YEARS OLD
MY client KATHERINE X has presented to our business/service/facility with the goal of lose weight as her GP suggest she
must exercise to reduce her health risk factors such as Type 2 Diabetes
KATHERINEinformation and measurements recorded during pre-exercise screening include the following:
Current
Physical
Activity level
NOT AT ALL
Sessions / week Notes:
─ TYPE 2 DIABETES
─ BMI -OBESITY
─ HIGH BLOOD PRESSURE 145/91mmHg
─ UNDER MEDICATION
─
Minutes / week
Intensity
(low/mod/high/ vig)
Resting HR
Resting BP
Weight
VC001 College of Sports & Fitness - 11/05/2017- SISFFIT015
International College of Capoeira Pty Ltd trading as ’College of Sports & Fitness’ ABN 90 125 114 730/ Registered
Training Organisation 91345/ CRICOS Provider Code 03057C
Assessment 1- Portfolio (SISSFFIT015)
BMI 31.5
Waist Circ
In response to her screening results I am requesting your guidance in relation to Katherine condition to enable me to
ensure delivery of a safe and effective exercise program. KATHERINE NEED A EATING PROGRAM PLAN WICH WILL HELP
HER TO REDUCE HER BODY WEIGHT AND REDUCE RISK FACTORS AS SUCH SHE IS SUFFER OF
Based on Katherine goals, I intend to have /her commence an exercise program consisting of the following:
Describe the intended program focus in brief strength / cardio based program; group vs 1:1
Please assess Katherine condition and indicate any recommendations you may have in relation to her exercise program,
including specific activities /she cannot or should not be undertaking at this time, or other relevant notes.
Bicycling: Cardio based blood pressure reducing program
Aerobics in alternative days: Fat burning exercises
Climbing stairs
Jogging: Locomotion as well as Cardio based program to enhance bone and muscle functions
Lateral pull downs
Lateral dumbbell raises
overhead presses work multiple muscles
I/ will keep you informed of KATHERERINE’s progress and any major changes in /her condition. To acknowledge you
have received this referral, please complete this section:
Date Referral received: 16/5/18 Status of Referral:
*please describe action required in notes Complete Incomplete*
Practitioner Name: KATE HOLMES Contact person for follow up:
**please provide new contact details in notes As above New contact**
Practitioner Title: DIETITIAN Notes:
Practitioner Signature: KATE HOLMES
Please include in notes any instructions you may have regarding follow up or progress reporting.
I/we welcome any advice you feel necessary and can be contacted by phone <123456789> during <9AM-5PM > or
email <ingidorth2@bigpond.coms> anytime.
VC001 College of Sports & Fitness - 11/05/2017- SISFFIT015
International College of Capoeira Pty Ltd trading as ’College of Sports & Fitness’ ABN 90 125 114 730/ Registered
Training Organisation 91345/ CRICOS Provider Code 03057C
BMI 31.5
Waist Circ
In response to her screening results I am requesting your guidance in relation to Katherine condition to enable me to
ensure delivery of a safe and effective exercise program. KATHERINE NEED A EATING PROGRAM PLAN WICH WILL HELP
HER TO REDUCE HER BODY WEIGHT AND REDUCE RISK FACTORS AS SUCH SHE IS SUFFER OF
Based on Katherine goals, I intend to have /her commence an exercise program consisting of the following:
Describe the intended program focus in brief strength / cardio based program; group vs 1:1
Please assess Katherine condition and indicate any recommendations you may have in relation to her exercise program,
including specific activities /she cannot or should not be undertaking at this time, or other relevant notes.
Bicycling: Cardio based blood pressure reducing program
Aerobics in alternative days: Fat burning exercises
Climbing stairs
Jogging: Locomotion as well as Cardio based program to enhance bone and muscle functions
Lateral pull downs
Lateral dumbbell raises
overhead presses work multiple muscles
I/ will keep you informed of KATHERERINE’s progress and any major changes in /her condition. To acknowledge you
have received this referral, please complete this section:
Date Referral received: 16/5/18 Status of Referral:
*please describe action required in notes Complete Incomplete*
Practitioner Name: KATE HOLMES Contact person for follow up:
**please provide new contact details in notes As above New contact**
Practitioner Title: DIETITIAN Notes:
Practitioner Signature: KATE HOLMES
Please include in notes any instructions you may have regarding follow up or progress reporting.
I/we welcome any advice you feel necessary and can be contacted by phone <123456789> during <9AM-5PM > or
email <ingidorth2@bigpond.coms> anytime.
VC001 College of Sports & Fitness - 11/05/2017- SISFFIT015
International College of Capoeira Pty Ltd trading as ’College of Sports & Fitness’ ABN 90 125 114 730/ Registered
Training Organisation 91345/ CRICOS Provider Code 03057C
Assessment 1- Portfolio (SISSFFIT015)
Client Consent: I give my permission for Professional/Business to communicate with the referring Practitioner
and/or my GP regarding my health status and my progress relating to my exercise program.
Client Name: Katherine x
Client Signature: Katherine x Date:16/5/18
Your Sincerely,
Marianna Sofianidou
Contact Name
Business Name fitness for well-being
Phone: Your Phone Number
Email: mariannasofianidou@gmai.com
Postal Address 71 Meredith street
Suburb Bankstown State NSW Postcode 2200
Business/Facility Opening Hours 9am-5pm
Part D
Portfolio – Make referrals (15 marks)
You are to demonstrate a collection of evidence in a portfolio showing your ability to identify and
refer clients requiring medical or allied health professional expertise. This task is most suited to
students currently working in the fitness industry and who have been working collaboratively with
medical and allied health professionals; however, your trainer may provide you with simulations as
deemed appropriate, especially for those who have not had sufficient access to the required
situations. Follow the instructions carefully to ensure you complete this task to the detailed level
required. You will need to provide a variety of evidence, such as supervisor reports, letters, DVD
recordings and so on. This assessment will need to be performed over a period of time to ensure you
have adequate time to provide the evidence of competency required.
Task:
VC001 College of Sports & Fitness - 11/05/2017- SISFFIT015
International College of Capoeira Pty Ltd trading as ’College of Sports & Fitness’ ABN 90 125 114 730/ Registered
Training Organisation 91345/ CRICOS Provider Code 03057C
Client Consent: I give my permission for Professional/Business to communicate with the referring Practitioner
and/or my GP regarding my health status and my progress relating to my exercise program.
Client Name: Katherine x
Client Signature: Katherine x Date:16/5/18
Your Sincerely,
Marianna Sofianidou
Contact Name
Business Name fitness for well-being
Phone: Your Phone Number
Email: mariannasofianidou@gmai.com
Postal Address 71 Meredith street
Suburb Bankstown State NSW Postcode 2200
Business/Facility Opening Hours 9am-5pm
Part D
Portfolio – Make referrals (15 marks)
You are to demonstrate a collection of evidence in a portfolio showing your ability to identify and
refer clients requiring medical or allied health professional expertise. This task is most suited to
students currently working in the fitness industry and who have been working collaboratively with
medical and allied health professionals; however, your trainer may provide you with simulations as
deemed appropriate, especially for those who have not had sufficient access to the required
situations. Follow the instructions carefully to ensure you complete this task to the detailed level
required. You will need to provide a variety of evidence, such as supervisor reports, letters, DVD
recordings and so on. This assessment will need to be performed over a period of time to ensure you
have adequate time to provide the evidence of competency required.
Task:
VC001 College of Sports & Fitness - 11/05/2017- SISFFIT015
International College of Capoeira Pty Ltd trading as ’College of Sports & Fitness’ ABN 90 125 114 730/ Registered
Training Organisation 91345/ CRICOS Provider Code 03057C
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Assessment 1- Portfolio (SISSFFIT015)
1. Access information from at least three clients with health or medical concerns that require
medical or allied health professional expertise. Use pre-test screening information and seek
additional health information from the clients as required.
2. Analyse health information to determine the need for referral and guidance. Recommend the
client seek advice from medical or health professionals as required and arrange the referral with
permission, consent and within confidentiality and privacy standards.
3. Maintain a case management file with all documents, communication and collaboration with
medical and allied health professionals.
Part E
Portfolio – Case management (20 marks)
You are to demonstrate a collection of evidence in a portfolio showing your ability to be part of an
entire case management file for two different clients. The goal is to be part of a team that is
managing a client for a particular concern, such as recovery after a motor vehicle accident or other
injury, Type 2 diabetes management and so on. This should involve liaising with local medical and/or
allied health professionals. An example of an appropriate case may include, but are not limited to
the following:
● a pregnant client who has been referred to the gym for an exercise program during her
pregnancy
● a postmenopausal client who has been referred to the gym for a weight-bearing cardiovascular
program and a resistance program to minimise the risk of the onset of osteoporosis
● a client you have referred who has presented to the gym with risk factors warranting guidance
and clearance from a doctor. You then continue managing this client under the care and
supervision of a doctor or allied health professional.
Check your case management file is appropriate with your trainer before submission. You will need
to submit all necessary documentation to support your claims of competency.
Note: One of your cases should include receiving at least one referral, while the other case should
involve you making at least one referral. Some cases may involve more than one medical and/or
allied health professional. If the client is not officially ‘discharged’ from the medical and/or allied
health professional, the case should be managed for at least two months to ensure adequate time to
demonstrate competency in this task.
VC001 College of Sports & Fitness - 11/05/2017- SISFFIT015
International College of Capoeira Pty Ltd trading as ’College of Sports & Fitness’ ABN 90 125 114 730/ Registered
Training Organisation 91345/ CRICOS Provider Code 03057C
1. Access information from at least three clients with health or medical concerns that require
medical or allied health professional expertise. Use pre-test screening information and seek
additional health information from the clients as required.
2. Analyse health information to determine the need for referral and guidance. Recommend the
client seek advice from medical or health professionals as required and arrange the referral with
permission, consent and within confidentiality and privacy standards.
3. Maintain a case management file with all documents, communication and collaboration with
medical and allied health professionals.
Part E
Portfolio – Case management (20 marks)
You are to demonstrate a collection of evidence in a portfolio showing your ability to be part of an
entire case management file for two different clients. The goal is to be part of a team that is
managing a client for a particular concern, such as recovery after a motor vehicle accident or other
injury, Type 2 diabetes management and so on. This should involve liaising with local medical and/or
allied health professionals. An example of an appropriate case may include, but are not limited to
the following:
● a pregnant client who has been referred to the gym for an exercise program during her
pregnancy
● a postmenopausal client who has been referred to the gym for a weight-bearing cardiovascular
program and a resistance program to minimise the risk of the onset of osteoporosis
● a client you have referred who has presented to the gym with risk factors warranting guidance
and clearance from a doctor. You then continue managing this client under the care and
supervision of a doctor or allied health professional.
Check your case management file is appropriate with your trainer before submission. You will need
to submit all necessary documentation to support your claims of competency.
Note: One of your cases should include receiving at least one referral, while the other case should
involve you making at least one referral. Some cases may involve more than one medical and/or
allied health professional. If the client is not officially ‘discharged’ from the medical and/or allied
health professional, the case should be managed for at least two months to ensure adequate time to
demonstrate competency in this task.
VC001 College of Sports & Fitness - 11/05/2017- SISFFIT015
International College of Capoeira Pty Ltd trading as ’College of Sports & Fitness’ ABN 90 125 114 730/ Registered
Training Organisation 91345/ CRICOS Provider Code 03057C
Assessment 1- Portfolio (SISSFFIT015)
Task:
1. Identify information that needs to be recorded in the case management file.
Client Name:
Client Address:
Client Contact number:
Pathophysiological history of client:
Specific information about any pain or regular sufferings:
BMI, Blood pressure, Blood sugar, Cardiac condition and other health report:
Any previous or recent injuries:
Cardiac capacity and breath frequency:
2. Identify information that needs to be shared with medical or allied health professionals and
provide as required.
Pathophysiological history of client:
Specific information about any pain or regular sufferings:
BMI, Blood pressure, Blood sugar, Cardiac condition and other health report:
Any previous or recent injuries:
3. Maintain current, complete, accurate and relevant client records for each client contact.
Pathophysiological history of client:
Specific information about any pain or regular sufferings:
BMI, Blood pressure, Blood sugar, Cardiac condition and other health report:
Any previous or recent injuries:
Cardiac capacity and breath frequency:
VC001 College of Sports & Fitness - 11/05/2017- SISFFIT015
International College of Capoeira Pty Ltd trading as ’College of Sports & Fitness’ ABN 90 125 114 730/ Registered
Training Organisation 91345/ CRICOS Provider Code 03057C
Task:
1. Identify information that needs to be recorded in the case management file.
Client Name:
Client Address:
Client Contact number:
Pathophysiological history of client:
Specific information about any pain or regular sufferings:
BMI, Blood pressure, Blood sugar, Cardiac condition and other health report:
Any previous or recent injuries:
Cardiac capacity and breath frequency:
2. Identify information that needs to be shared with medical or allied health professionals and
provide as required.
Pathophysiological history of client:
Specific information about any pain or regular sufferings:
BMI, Blood pressure, Blood sugar, Cardiac condition and other health report:
Any previous or recent injuries:
3. Maintain current, complete, accurate and relevant client records for each client contact.
Pathophysiological history of client:
Specific information about any pain or regular sufferings:
BMI, Blood pressure, Blood sugar, Cardiac condition and other health report:
Any previous or recent injuries:
Cardiac capacity and breath frequency:
VC001 College of Sports & Fitness - 11/05/2017- SISFFIT015
International College of Capoeira Pty Ltd trading as ’College of Sports & Fitness’ ABN 90 125 114 730/ Registered
Training Organisation 91345/ CRICOS Provider Code 03057C
1 out of 18






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.